A 56-year-old man with infective endocarditis underwent mechanical prosthetic aortic valve implantation complicated by a large pseudoaneurysm of the left ventricular outflow tract (LVOT), which had been unsuccessfully treated by 2 previous surgical interventions. The patient was referred to our center for percutaneous closure of the pseudoaneurysm due to dyspnea and high surgical risk.
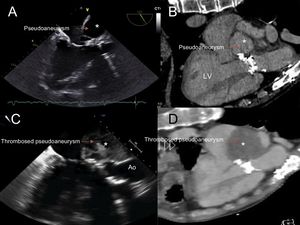
An echocardiogram demonstrated an LVOT pseudoaneurysm, and a computed tomography scan showed a mass of 10 × 8cm, connecting to the LVOT through a narrow 3-mm neck, adjacent to the anterior mitral valve. The mass was suggestive of a pseudoaneurysm (asterisk in Figure 1) based on contrast uptake in the late venous phase (Figure 1A and B [LV, left ventricle] and Video of the supplementary material).

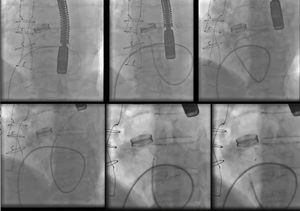
A transseptal (TS) approach to the left ventricle through femoral venous access was used due to the presence of a mechanical aortic prosthetic valve, thereby avoiding a more invasive transapical access. A catheter was placed in the right atrium, and a TS puncture was performed with extreme caution due to the risk of pseudoaneurysm rupture because of its giant size. Initially, a deflectable Fustar 9-Fr system was placed; however, this system did not allow the catheter to be guided toward the entrance of the pseudoaneurysm, and so it was replaced with a Destination 6-Fr. The wire was introduced to the cavity, and with the aid of a diagnostic 4-Fr catheter, an Amplatzer Vascular Plug-4 was successfully deployed (Figure 2).

At a 6-month follow-up, the patient was asymptomatic, and a computed tomography scan and echocardiogram showed almost complete thrombosis of the pseudoaneurysm (Figure 1C and D; Ao, aorta).
Conflicts of interestX. Freixa is proctor for St Jude Medical.