To the Editor:
The Rastelli procedure is considered to be the technique of choice for the treatment of transposition of the great arteries (TGA) with interventricular communication (IVC) and obstruction of the right ventricular outflow tract (RVOT).1-3 The procedure uses an intracardiac patch that directs the blood from the left ventricle (LV) to the aorta via the IVC, thereby achieving continuity between the right ventricle (RV) and the pulmonary artery by means of an extracardiac valved conduit.1 Lecompte et al4 described a similar operation using a patch instead of the valved conduit, which enables correction in small children but leaves a free pulmonary regurgitation.
The Nikaidoh procedure is an alternative in patients whose anatomy precludes the Rastelli procedure (small IVC and located away from the LVOT, multiple IVC, small RV, mitral-tricuspid straddling, cone-shaped implants of the tricuspid valve, or the anterior implant of the mitral valve).5,6 We present the case of the first child to undergo surgery in our hospital using the modified Nikaidoh procedure (with a Contegra conduit).
The patient was a boy with TGA, a high muscular IVC and pulmonary valve stenosis. At 11 days of age he underwent a Rashkind procedure and at 3 years of age a pulmonary valvuloplasty (catheterism). At 4 years of age he underwent surgery due to increased cyanosis. Dissection was made of the aortic and pulmonary roots and the coronary vessel origins. The pulmonary root of the LVOF was removed. The aortic root and the coronaries were extracted. The septal muscle was cut between the pulmonary root and the IVC. This left a large opening between the ventricles through which the aortic root was translocated to the LV, leaving a large IVC just below the aortic root in its new position, which was closed with a patch. The distal end of a Contegra conduit (18 mm) was anastomosed to the pulmonary bifurcation, which was then on the right of the aorta, and the extreme proximal end was sutured to the RV outflow orifice after enlarging the RVOT. The IVC was closed and the aorta unclamped. The post-surgery echocardiogram showed good contractility, mild mitral and tricuspid insufficiency, a residual IVC of 2-3 mm with no hemodynamic repercussions, laminar flow in both outflow tracts and minimal aortic and Contegra conduit failure. The patient was discharged 11 days after surgery. Eight months after the operation the patient remained asymptomatic (NYHA I).
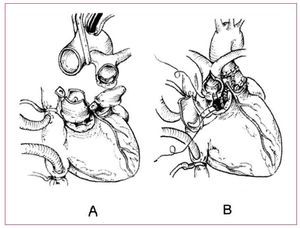
The Rastelli technique achieves good short-term results,1,6 but it is associated with important long-term disease, due to obstruction of the conduit and the LVOT (occurring in 10% of the patients because of the tendency of the IVC to close and the fact that the implanted tube is unable to grow) or due to arrhythmias, which necessitate the patient undergoing further surgery.5-7 In patients with an inadequate anatomy for the Rastelli procedure, aortic translocation, or the Nikaidoh procedure, may be an attractive option.5 The original technique consisted of translocating the aortic root to the LV without deinsertion of the coronary vessels.4 This can cause problems of coronary flow, which was why the coronary vessels were transferred.5 An anomalous coronary anatomy may be a contraindication for this technique.5 The Nikaidoh procedure achieves a more anatomic reconstruction and it can be applied to TGA with different anatomic variants.1 Figure shows a representation of the modified Nikaidoh procedure.

Figure. Modified Nikaidoh procedure. The ascending aorta and the pulmonary trunk are sectioned. The coronary arteries are deinserted. The interventricular communication is closed and the aortic root translocated to the LVOT, the pulmonary root to the RVOT and the coronary arteries are reimplanted.
Considering that the reestablishment of the normal cardiac anatomy is the standard in surgery for congenital heart disease, the modified Nikaidoh procedure may in the future replace the Rastelli technique. A long-term follow-up is required to determine the possible complications and the evolution of patients who undergo surgery with this technique.