To the Editor:
Radiotherapy and hypothyroidism are unusual causes of acquired atrioventricular block (AVB). Thoracic radiotherapy used for the treatment of different neoplasms may cause adverse cardiac1,2 and endocrinologic3 events, attributed to fibrosis of the conduction tissue and the thyroid gland, respectively. The infra-Hisian localization of an AVB is uncommon in young patients, but nevertheless of great clinical importance, given its prognostic implications. We report a patient with infra-Hisian AVB and hypothyroidism, both of which had developed progressively 17 years after receiving radiotherapy for a Hodgkin lymphoma.
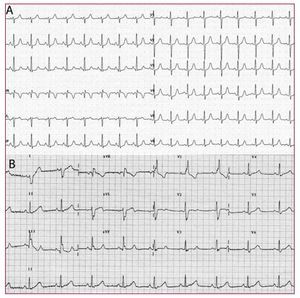
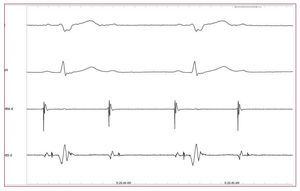
The patient was a 36-year-old woman, with a history of Hodgkin lymphoma diagnosed at the age of 19 years and treated with chemotherapy, Mantle-type radiotherapy (48 Gy) and an autologous bone marrow transplant, which had been in complete remission for 15 years. In 2000 she was diagnosed with hypothyroidism, attributed to glandular fibrosis resulting from the radiotherapy. Since 2003 she had required replacement therapy, with good subsequent control. She was referred to the cardiology service due to palpitations lasting several hours associated with situations of emotional stress, of sudden onset and gradual end. Physical examination, laboratory tests (including the thyroid profile), and an echocardiogram were all normal. An electrocardiogram showed sinus rhythm with first degree AVB, left posterior hemiblock and right bundle branch block, with a clear progression of the conduction disorder as compared with an electrocardiogram done 6 years previously (Figure 1). The Holter showed a Mobitz II second degree AVB during the moments of maximum heart rate and a 2:1 AVB during an episode of clinical palpitations. The electrophysiologic study showed severe involvement of the infra-Hisian conduction (HA, 67 ms; HV, 68 ms), with frequent P waves spontaneously blocked at the infra-Hisian level (Figure 2). Given the Mobitz II second degree AVB and the bifascicular block, a bi-chamber pacemaker was implanted.

Figure 1. A: electrocardiogram 6 years before admission. B: electrocardiogram on admission with palpitations, 2:1 atrioventricular block and bifascicular block.

Figure 2. Recording of the electrophysiologic study showing infra-Hisian 2:1 atrioventricular block.
Acquired AVB in young patients is a very exceptional disorder. The patient presented here had two factors that might account for the AVB: radiotherapy and hypothyroidism.1,2,4,5
Atrioventricular block secondary to hypothyroidism4 is an unusual entity that is due to the myxedematous infiltration of the conduction tissue and which presents as one more symptom amongst many, in which the onset of AVB is relatively early, even during phases of sub-clinical hypothyroidism. The localization of the block is mainly supra-Hisian6 (first degree or Mobitz I AVB) and in many cases it can be successfully reverted with replacement therapy.4
In patients with AVB and a history of radiotherapy, biopsy studies reveal a severe, progressive fibrosis5 of the conduction tissue as the main cause of the block. The history of radiotherapy usually dates back a long time (15-20 years), which can thus sometimes make the association with AVB more difficult to suspect.1,2 The electrophysiologic study enabled the block to be localized as infra-Hisian in most published reports.5 Its evolution is irreversible and requires implantation of a pacemaker.
The progressive nature of the block seen on the evolution of the electrocardiograms, the absence of other symptoms and signs of hypothyroidism, the normal thyroid function with replacement therapy and the infra-Hisian localization all point to the radiation as the most likely cause.
Although this type of radiotherapy is no longer used, many patients have received it over the past decades. Periodic electrocardiograms are therefore recommended in the follow-up of these patients, bearing in mind the slow but progressive evolution of the fibrosis and the AVB.
The case presented here poses the differential diagnosis between 2 unusual etiologies of AVB and stresses the importance of regular electrocardiograms and a good clinical history for a correct diagnosis.