To the Editor,
Aortic infection, or aortitis, is a rare entity that can lead to aneurysm or mycotic pseudoaneurysm formation. It affects patients with aortic arteriosclerosis or simultaneous infective endocarditis,1 and is rare in patients without these predispositions. Moreover, while aortic wall infection can lead to aneurysmatic dilatation, it is much more common for a previously dilated vessel to become infected.1 The most frequently isolated microorganisms are species of Staphylococcus, Enterococcus and Streptococcus pneumoniae.1 The healthy aortic wall is infected by microorganisms like Staphylococcus aureus and Salmonella species.1 Infection by Candida is extremely rare, occurring in <1% of cases.2, 3
A 72-year-old patient was admitted to the coronary unit with signs and symptoms compatible with fully evolved, inferoposterior acute myocardial infarction and no previous cardiologic history. He had attended the emergency room for a bout of dizziness and reported having presented precordial oppression 48h earlier that irradiated to the left upper extremity. The electrocardiogrampresented Q waves of necrosis in lower leads and an R greater than S in the V2 lead. Analyses found troponin elevation with normal creatine kinase, which explains why he was admitted to the coronary unit with a diagnosis of fully-evolved inferoposterior myocardial infarction. Transthoracic echocardiography revealed conserved function and posterior and inferior, mid and basal, akinesia. Furthermore, right paracardiac images showed dense liquid –increasingly dense in the interior– severely compressing the right atrium (Figure 1). Consequently, thoracic computerized tomography (CT) was performed. This revealed an aortic root pseudoaneurysm communicating with the pericardiac cavity where there was a hematoma, showing images of air in its interior compatible with superinfection (Figure 2). We interpreted this as a mycotic aortic pseudoaneurysm over a nonaneurysmatic aorta contained by the pericardium and likely to compromise the right coronary artery. Given the echocardiographic signs of partial right cavity collapse, we decided on urgent cardiovascular surgery to decompress the cavities and repair the aortic wall defect. Thoracic CT revealed an extensive calcification at the level of the left coronary artery and descending anterior artery. However, we ruled out catheterization prior to the intervention as we considered the risk too high. We did consider using multislice CT but it was unavailable. During the intervention, hematoma and a large quantity of pus escaped when the pericardium was opened. Both pericardium and myocardium were swollen and infiltrated. We identified two sites of aortic rupture in the ascending aorta anterior wall and repaired them with pericardium. Candida albicans grew in cultures of the samples extracted during the intervention. Antifungal therapy was completed. After 1 month hospitalization in our center, the patient was discharged in good condition, which continued at the 1-year follow-up.

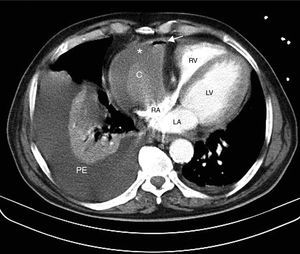
Figure 1. Thoracic computerized tomography image showing aortic pseudoaneurysm. There is a hematoma in the pericardium (*) with a clot inside it (C) that presents bubbles of air (arrow). The right atrium is compressed. Pleural effusion more dense than water, signs of blood or pus, and pulmonary atelectasia of the right inferior lobar artery. LA, left atrium; LV, left ventricle; PE, pleural effusion; RA, right atrium; RV, right ventricle.

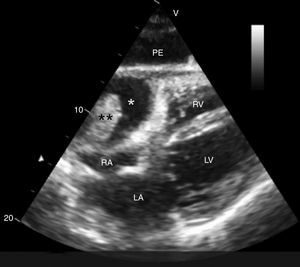
Figure 2. Transthoracic echocardiogram subcostal plane showing right paracardiac image of dense liquid (*), with solid image in its interior (**), all of which is related with pseudoaneurysm communicating with a partially thrombotic pericardium. This rejects and severely compresses the right atrium. The pleural effusion is also revealed. LA, left atrium; LV, left ventricle; PE, pleural effusion; RA, right atrium; RV, right ventricle.
To conclude, mycotic pseudoaneurysm is an extremely rare infection that can occasionally have atypical manifestations. Hence, we must be especially alert to achieve early diagnosis that will permit appropriate treatment and thus reduce the risk of mortality it entails.
Corresponding author: Arantza.manzanal@gmail.com