Keywords
INTRODUCTION
The study of contractile reserve (CR) of the left ventricle (LV) using low-dose dobutamine (LDD) has been used to study myocardial viability via different techniques.1-15
Improvement in the thickening and contractility of highly hypokinetic or akinetic segments at rest, when using LDD, has been taken as a specific criterion of myocardial viability, supported by the general improvement in ejection fraction (EF). However, changes in EF might be partly affected by improvements in other segments not included in the viability diagnosis, such as those with mild or moderate hypokinesia at rest, and even by the possibility of contractility worsening in other segments. This point, which has not been addressed in other publications on the subject, means that the final interpretation of the images acquired while using LDD is not as simple as it might seem a priori.
Numerous studies have assessed dobutamine infusion using echocardiography to predict the behavior of segments with highly anomalous contractility after revascularization as well as the prognosis of patients based on viability criteria.16-18 However, the literature on myocardial perfusion gated-SPECT—a technique that evaluates perfusion and allows the study of the thickening and displacement of all LV segments—is more scarce4-10 and no detailed analyses have been made of segmental patterns using LDD and its relationship with the overall response of left ventricular systolic function. This prospective multicenter study attempts to fill this gap. It was conducted in patients with ischemic heart disease, where the study of myocardial viability has greater clinical relevance.
METHODS
Patients
A total of 89 consecutive patients were studied using myocardial perfusion gated-SPECT at rest and during LDD infusion. The selection criteria, according to the referring cardiologist in charge, were clinical indication of gated-SPECT in patients with a diagnosis of chronic ischemic cardiomyopathy confirmed by previous myocardial infarction and coronary angiography (multivessel disease with coronary stenosis ≥50%), LVEF £40% during myocardial perfusion gated-SPECT at rest, and <75 years old. The diagnostic criteria for myocardial infarction were those recommended in the clinical guidelines on infarction of the European Society of Cardiology.19 Exclusion criteria included mechanical complications arising from the infarction, previous coronary revascularization, and the presence of another disease with a poor short-term prognosis.
Design
This was a multicenter prospective study in which 8 tertiary care hospitals participated. Patients who had been initially evaluated with myocardial perfusion gated-SPECT for medical reasons and fulfilled the selection criteria were asked to attend a new appointment and signan informed consent before 10 days had passed since the previous test in order to undergo gated SPECT at rest and with LDD. All centers performed image acquisition in the same way. Image interpretation and statistical tests were performed in the imaging unit of the coordinating center. This study was approved by the hospital's ethical committee on clinical trials.
Gated SPECT With Low-Dose Dobutamine
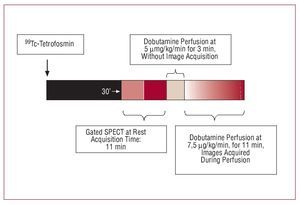
First, a dose of 740-925 MBq of 99Tc-tetrofosmin was injected at rest, and 30 min later acquisition was performed at rest. Once this was completed, an infusion of 5 µg/kg/min dobutamine was initiated lasting 3 min. A second gated-SPECT acquisition procedure was then performed at the same time as increasing the dobutamine dose to 7.5 µg/kg/min. After 11 min, both image acquisition and dobutamine infusion ended (Figure 1). Continuous ECG monitoring was performed and systemic blood pressure checked every 3 min.

Figure 1. Sequence of gated-SPECT studies at baseline and with low-dose dobutamine.
Images were acquired with gamma cameras provided with a high-resolution collimator, following a semi-circular orbit starting at 30o right anterior oblique view with capture every 3o ending after a 180o turn at the left posterior oblique view. Images were reconstructed using a 5th-order Butterworth filter at a 0.4 cutoff frequency. Images were obtained in the short axis, horizontal long axis, and vertical long axis. Interobserver variability and variability between the EF estimates calculated with gated-SPECT were 0.5 (2.6) and 2 (5.1) EF points, respectively.20
Quantification of Segmental Thickening
The left ventricle was divided into 17 segments, each of which had a score assigned depending on its level of activity (0, normal perfusion; 1, light hypoperfusion; 2, moderate hypoperfusion; 3, severe hypoperfusion; and 4, no uptake). Two observers blinded to the patients' clinical characteristics and the conditions under which gated-SPECT was performed made a quantitative analysis of each segment consensually assigning them a given score based on contractility and thickening (0, normal; 1, mild reduction; 2, moderate reduction; 3, severe reduction; and 4, none). Similarly, EF and ventricular volumes (end-systolic volume [ESV] and end-diastolic volume [EDV]) were quantified under gated-SPECT at rest using QGS methodology.21 Contractile reserve was assumed to be present when, during LDD infusion, the thickening score improved by at least 1 point compared to at rest.22
After analyzing the thickening of each segment during LDD infusion, an index was created to analyze the global effects of increased and reduced thickening on the 17 LV segments during an increase in EF ≥5%. This index, called the general thickening index (GTI), expresses the relationship between the number of segments with increased thickening (A) and the number of segments with reduced thickening (B) in relation to the total LV area: (A-B/17)´100. The following were calculated: positive GTI (predominance of segments with increased thickening), negative GTI (predominance of segments with reduced thickening), and neutral GTI (the same number of segments with increased and reduced thickening).
Statistical Analysis
Discrete variables are expressed as percentages and continuous variables as means, with their respective standard deviations. The c2 test was used to compare 2 independent discrete variables; when the number of expected individuals in one or more cells of the contingency table was <5, Fisher's exact test was used.
The Student t test for paired data was used to analyze the continuous variables of gated-SPECT at rest and with LDD. The Student t test for independent samples was used to analyze the continuous variables of patients with or without an increase in EF ≥5%. Thickening behavior during LDD infusion was analyzed using linear regression and binary logistic regression.
At the end of the study, 2 multiple logistic regression models were constructed. A step inclusion method (FSTEP-LR) was used based on the likelihood ratio (input, P=.05; output, P=.10). The variables introduced were statistically significant in the univariate analysis (P<.05) and by clinical criteria. The predictive value of each model was assessed with the ROC curve (receiver operating characteristic) with a 0.5 cutoff point for classification.
All variables analyzed were introduced into a database created with SPSS (version 15, SPSS, Chicago, Illinois, USA). A P value less than .05 was considered significant.
RESULTS
Table 1 shows the general clinical characteristics of patients at baseline. A total of 82 (92.15%) patients had a history of myocardial infarction: 60 had 1 infarction, 20 had 2, 1 had 3, and 1 had 4 infarctions.

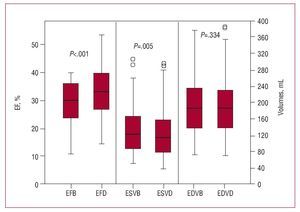
During LDD infusion, a significant increase was observed in EF and a reduction in left ventricular ESV (Table 2, Figure 2). In 33.7% (30) of patients, the increase in EF was ≥5% and in 5.6% (5) EF decreased by ≥5%.


Figure 2. Box diagram showing ejection fraction (EF) values at baseline (EFB) and with dobutamine (EFD), and end-systolic and end-diastolic volumes at baseline (ESVB and EDVB) and with dobutamine (ESVD and EDVD). The upper borders of the boxes correspond to the 75th percentile; the lower borders, to the 25th percentile; and the central marks to the 50th percentile. Significant differences were found between EFB and EFD, and between ESVB and ESVD.
At baseline, under gated-SPECT, 65.8% (996) of the segments presented thickening abnormalities (8.33%, mild abnormalities [grade 1], 12.03%, moderate abnormalities [grade 2], and 45.47%, severe abnormalities [grade 3-4]). In the LDD study, an improvement in thickening was observed in 181 (12%) of the 1513 segments analized, and worsening in 101 (6.6%). An improvement in thickening was observed in 18.2%, 22.5%, 17.6%, and 16.9% of the segments with grade 1, 2, 3, and 4, respectively, and worsening in 7.7%, 11.1%, 10.9%, and 8.05% of the segments with grade 0, 1, 2, and 3, respectively.
Association Between Segmental Thickening and Ventricular Volumes
An optimal cut-off point was calculated using ROC curves (£10 ml; ROC=0.77, 95% confidence interval [CI] 0.67-0.85; sensitivity, 63.3%; specificity, 81.4%; positive predictive value, 63.4%; negative predictive value, 81.4%; positive likelihood ratio = 3.4) for ESV changes which were associated with a significant increase in EF. The improvement in grade 3-4 thickening significantly decreased ESV (£10 mL) during LDD infusion (adjusted odds ratio [OR] = 2.8 [95% CI, 1.1-7.1]; P=.034), whereas improvements in grades 1-2 did not have a significant influence (adjusted OR = 1.7 [95% CI, 0.7-4.6]; P=.260). Changes in EDV were not significantly related to increases in EF.
Association Between Segmental Thickening and Ejection Fraction
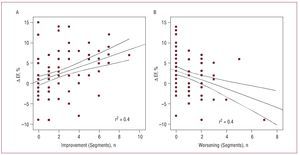
In the linear regression analysis (adjusted for segments with worsened thickening and for normal segments with no change), a linear and significant relationship was observed (ANOVA, F=8.283; adjusted R2=0.2; P<.001; b=1.04 [95% CI, 0.38-1.7]) between the total number of segments with improved thickening and EF difference (D EF). In particular, the segments with improved thickening increased the EF by 1.04% per each improved segment (Figure 3A), whereas a significant negative linear relationship was found for the total segments with worsened thickening (b=-1.1 [95% CI, from -1.7 to -0.38]; P=.003) (Figure 3B). Thus, the effect of segments with worsened thickening after LDD infusion decreased the EF by 1.1% per each worsened segment.

Figure 3. A: in the regression analysis, a significant linear and positive relationship was found between the number of segments with improved thickening with dobutamine and the increase in ejection fraction (D EF = EF with low-dose dobutamine - baseline EF). B: a significant linear and negative relationship was found between the number of segments with worsened thickening with dobutamine and a decrease in EF D. Dotted lines correspond to the 95% CI for the population.
In the binary logistic regression analysis, improved thickening in grade 3-4 segments, once adjusted for improvements in grade 1-2 segments, had an OR=18.3 (95% CI, 5.3-63; P<.001), and improvement in grade 1-2 segments, after adjusting for improvement in grade 3-4 segments, had an OR=4.5 (95% CI, 1.3-16; P=.02).
For an EF increase ≥5%, the optimal cut-off point obtained using ROC curves for segments with grade 3-4 thickening at baseline that improved during LDD infusion was ≥3 segments, and for improved grade 1-2 segments this was ≥10 segments (Table 3).

Subsequently, positive, negative and neutral GTI was analyzed among the patients with or without an EF increase ≥5% (Table 4). Patients with an EF increase ≥5% had a significantly greater positive GTI, whereas neutral GTI was more significant in the patients without a significant increase in EF.

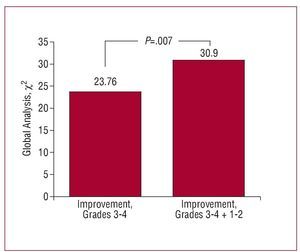
In order to analyse the variable predictive of significant improvement in EF, we used a binary logistic regresion model introducing the following variables: improvement in at least 3 segments with severe thickening abnormalities, improvement in at least 10 segments with mild-moderate abnormalities, the number of segments with reduced thickening, and ESV and EDV. In the first step, the independent predictive variable (adjusted for age and sex) was improvement in at least 3 segments with severe thickening abnormalities (OR=18.43 [95% CI, 5.1-66.5]; χ2=19.778; P<.001), and in the second and last step, improvement in at least 10 segments with mild-moderate thickening abnormalities was added (OR=4.53 [95% CI, 1.26-16.16]; c2=5.409; P=.02) (specificity, 84.7%; sensitivity, 70%; efficiency, 78.7%). Grade 1-2 segments with improved thickening presented a significant incremental value (P=.007) in the likelihood of the model (Figure 4).

Figure 4. Incremental value (defined by the general c2 statistic) of improvement (with dobutamine) in the segments with grade 1-2 thickening at baseline compared to improvement in segments with grade 3-4 thickening at baseline, for an increase in ejection fraction ≥5%.
DISCUSSION
In the present study, LDD infusion in 89 patients with ischemic heart disease and systolic dysfunction led to an increase in EF ≥5% in 33.7% of patients, whereas there was a reduction ≥5% in 5.6%. The increase in EF was accompanied by a significant reduction in ESV and smaller reductions in EDV, similar to the findings of Everaert et al.23 The reduction in EF could be explained by the induction of silent ischemia (supply-demand imbalance), the increase in intraventricular pressure (diffuse subendocardial ischemia), or the increase in left ventricular remodeling due to the increase in the contractility of the segments with normal thickening that pull and dilate the infarct area during dobutamine infusion and aggravate the contractile function (non-ischemic reduction of ventricular function).
The improvement in grade 3-4 thickening significantly reduced ESV during LDD infusion, and the reduction in ESV ≥10 mL was significantly associated with an increase in EF ≥5%, at a cutoff value obtained with ROC curves. The behavior of ventricular volume indicates the effect of contractile reserve on reducing ventricular remodeling during LDD infusion.
The increase in the total number of segments with improved thickening increased the EF by 1.04% per each improved segment, whereas the increase in the number of segments with worsened thickening reduced the EF by 1.1% per each aggravated segment. The improvement in thickening in grade-3 segments had the most significant influence on the increase in EF. These results are similar to those obtained in patients studied using contrast ventriculography and LDD24 and dobutamine stress echocardiography,22 although this type of examination (unlike gated-SPECT) makes it possible to assess the so-called 2-phase response (improved contractility with LDD and worsening upon increasing the dose). In our series, the cutoff point for the segments with severe thickening alterations was smaller (at least 3 segments) compared to those which presented mild-moderate alterations (at least 10 segments). The increase in EF also had an influence, although to a smaller extent, on the improvement in thickening in grade 1-2 segments, which are not usually selected for studying viability.
The effect on EF of the segments with reduced thickening after LDD administration was probably caused by induced myocardial ischemia. It has been found that negative contractile reserve (defined as worsening contractile function with LDD compared to at rest) can indicate myocardial ischemia. Thus, negative and positive contractile reserve (sign of stunning or hibernation) both predict with equal reliability contractile recovery after revascularization.6 Furthermore, in 2-dimensional echocardiographic studies the negative component of the 2-phase response in myocardial contractility has been attributed to myocardial ischemia, with equal prevalence among stunned segments and hibernating segments.22
The GTI associates the combined interaction of the segments with different grades of contractile reserve during LDD infusion with the increase in EF ≥5%. In the multivariate model used to study the variables predicting significant improvement in EF, it was found that both the improvement in at least 3 segments with severe thickening alterations and the improvement in at least 10 segments with mild-moderate thickening alterations and a positive GTI were predictors of a significant increase in EF.
With the aim of establishing a diagnosis of myocardial viability, different studies with a small number of patients have analyzed LV contractile reserve using LDD infusion echocardiography,2,3 gated-SPECT4-6,8-15 and magnetic resonance imaging.1,25 Myocardial perfusion gated-SPECT makes it possible to assess segments poorly visualized using echocardiography8 and, in some series, has been found to be more powerful in predicting recovery from myocardial dysfunction after revascularization than echocardiography when 2 viability markers are associated, such as cellular integrity assessed by the degree of radionuclide uptake and contractile reserve assessed by LDD infusion.14 However, most studies on myocardial perfusion gated-SPECT using LDD have been limited to comparing changes in myocardial thickening with baseline perfusion values and only in the segments with severe contractility abnormalities.
Analyzing contractility and LV thickening together is complex, and although improved thickening using LDD in a segment is synonymous with its viability, the relationship between the behavior of the LV segments as a whole, EF evolution and ventricular volume is less clear. This is particularly important for the prognosis of patients who have undergone revascularization for ischemic heart disease, because prognosis largely depends on the improvement in EF after revascularization. Evidence showing that LVEF can decrease in some patients during LDD infusion has not been reported in previous publications. In patients with reduced systolic function and high ventricular volumes, in whom the criteria for predicting improvement in EF after revascularization are ambiguous,26 knowledge concerning the changes in these parameters during LDD infusion has obvious clinical relevance.
CONCLUSIONS
The behavior of LV systolic function in ischemic heart disease when using LDD is not only affected by the contractile reserve of the segments with reduced systolic thickening at baseline, but also by the worsening that can be found in 6.6% of the other segments. On the other hand, the increase in systolic function is associated not only with the improvement in the segments with very reduced thickening, but also with the improvement in the segments with mild-to-moderate reduced thickening. The improvement in the latter also has incremental predictive value regarding the increase in EF, whereas those that worsen also have an influence. Although these conclusions may seem predictable, and even obvious, their clinical importance is not insignificant, since the interpretation of these studies is relevant to deciding whether or not a patient should undergo revascularization.

ABBREVIATIONS
CR: contractile reserve
FE: ejection fraction
GTI: general thickening index
LDD: low-dose dobutamine
LV: left ventricle
SPECT: single-photon emission computerized tomography
The Appendix includes a list of the RECAVA researchers who participated in this study.
This study was partially financed by Redes temáticas de enfermedades cardiovasculares from the Carlos III Institute (Red C03/01, RECAVA).
Correspondence: Dr. J. Candell-Riera.
Servei de Cardiologia. Hospital Universitari Vall d'Hebron. Universitat Autònoma de Barcelona.
Pg. de la Vall d'Hebron, 119-129. 08035 Barcelona. España.
E-mail: jcandell@vhebron.net
Received February 19, 2008.
Accepted for publication May 27, 2008.