To the Editor:
Hypertrophic cardiomyopathy is the most common cause of sudden cardiac death in adults under 35 years of age.1 The annual mortality rate is estimated to be approximately 1%, and at least half of these deaths occur suddenly.2 According to the Spanish Implantable Cardioverter-Defibrillator Registry, hypertrophic cardiomyopathy is the underlying disease in 6% of the patients with implantable cardioverter-defibrillators (ICD).3 Given that sudden death can be the first sign of the disease and that this occurs most often in adolescents and young adults,4 it would appear to be necessary to establish adequate risk stratification criteria. Thus, we have read the work of Marín et al5 on the characteristics of patients with this cardiomyopathy who underwent cardioverter-debrillator implantation and their analysis of the results of this treatment with great interest. In this respect, we would like to report the experience at our center in a similar group of patients and their long-term follow-up.
Of a series of 216 patients who underwent implantation of 276 ICD between October 1991 and December 2004, 14 patients had been diagnosed as having hypertrophic cardiomyopathy. In five patients (35.7%), the indication for implantation was secondary prevention (two with resuscitated sudden death and three [64.3%] with sustained ventricular tachycardia) and in nine patients, it was primary prevention (six patients with syncope, two of whom presented no other risk factors, and three patients with at least two of the other risk factors associated with an increased risk of sudden death). In the article by Marín et al,5 4.4% of the patients presented a single risk factor as the indication for implantation, versus 14.28% in our series who received an ICD for this reason. However, as Maron established in his editorial,6 the conservative strategy followed by European centers, including those in Spain, which involves the application of primary prevention only in patients with two risk factors means that there are high-risk patients in whom the implantation of an ICD is not an option.
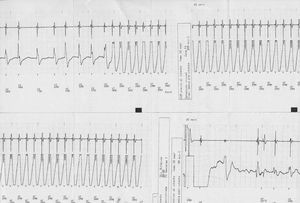
Over a follow-up period of 54.2 (39.8) months, five patients (35.7%) received an appropriate shock from the system (Figure), 3 of them in secondary prevention (60%) and 2 patients in primary prevention (22.2%). Neither of the two patients with a single risk factor received a shock from the system, although there is often a prolonged delay between ICD implantation and the first appropriate intervention in patients with this disease.

Figure. Electrogram recorded by one of the implantable cardioverter-defibrillators showing an episode of ventricular tachycardia in which the shock delivered by the system was appropriate and effective.
Two patients (14.3%) received inappropriate shocks, due to oversensing in one case and to episodes of rapid atrial fibrillation in the other.
There were no deaths and no patient required heart transplantation during the follow-up period.
Although with the limitations inherent in such a small series of patients, our experience confirms the high rate of appropriate therapies in secondary prevention (60%) and an appreciable rate in primary prevention (22.2%). The rate of appropriate therapies in primary prevention was higher in our series (22.2% over a follow-up period of 54 months), as compared with that reported by Marín et al (3.7% in 32 months).5
The ICD is an effective device for the prevention of sudden death in patients with hypertrophic cardiomyopathy. Future studies will establish the indications in the primary prevention setting, especially in patients with a single risk factor.