
To the Editor:
We report on a 45-year-old patient with no history of heart disease who presented at the cardiology unit after experiencing 2 months of effort angina episodes. Cardiovascular risk factors included high blood pressure, type 2 diabetes mellitus treated with oral agents, dyslipidemia, being an ex-smoker, and a family history of death from acute myocardial infarction. Physical examination, chest radiography, and analytics were compatible with normality. The electrocardiogram showed a Q wave and negative T wave in DIII.
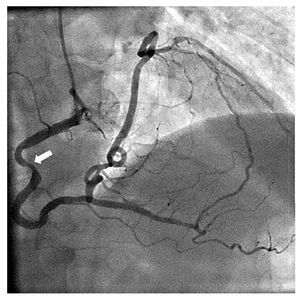
An exercise test using the Bruce protocol case gave positive clinical and electrical findings with a high-risk pattern from the second minute. Given these findings, the patient was admitted as a priority case for coronary angiography. The study was performed via the right radial artery and showed an anatomical variant of the coronary tree with single coronary output from the right coronary (RC) ostium in the right coronary sinus, left main agenesis, and hypoplasia of the left anterior descending branch. The segment corresponding to the RC followed the usual anatomical route and, through one of the posterolateral trunks, provided anterograde flow to the circumflex, marginal and bisector branch, as well as to the descending anterior hypoplastic, which also received flow from a right atrial branch. Both the left anterior descending and circumflex followed their normal anatomical route. There was a serious injury of 70% stenosis in the proximal segment of the RC, which was interpreted as being equivalent to a common trunk injury and as explaining the patient's chart. A 70% injury was also shown in the third bisecting proximal branch (Figure 1). Left ventricular systolic function was preserved without segmental alterations in contractility, and ejection fraction was 68%.

Figure 1. Angiography. Single coronary artery running from the right coronary sinus. The arrow indicates the severe injury to the proximal third.
A 64-slice multidetector computed tomography (CT) was used to complete the study and confirmed the conventional coronary angiography findings of the absence of the left coronary ostium. The segment affected in the middle third of the RC showed complicated-looking plaque with fibrocalcific content, which produced severe stenosis (Figure 2).

Figure 2. Multislice computed tomography. The arrow on the left indicates the fibrocalcific component of the complicated plaque in the single proximal coronary artery. On the right, a rendered reconstruction where the absence of the left main trunk can be observed.
The decision was made to implant a zotarolimus 4/20 mm stent in a percutaneous intervention. The success of the implant was confirmed using intravascular ultrasound. Following discharge, the patient was asymptomatic. Exercise testing was repeated 2 months after the procedure with negative clinical and electrical results after 11 min of effort.
Several series have described an incidence of coronary artery anomalies of around 1% in patients undergoing coronary arteriography.1 Most of these abnormalities are not associated with the appearance of symptoms, signs or poor prognosis and are often incidental findings. However, some anatomical variants involve a greater risk of sudden death or complications and require a precise diagnosis and surgical correction, if applicable. One such anomaly is the isolated single coronary artery.2
Our case corresponds to an R-I-a variant of the classification proposed by Lipton et al,3 and is one of the rarest patterns.1 In their review,4 Barriales et al described the possible complications of these anomalies, principally sudden death and induced ischemia even in the absence of atherosclerosis. For that reason, they recommended imaging and ischemia tests to identify the highest risk patients.
The case described is a high-risk coronary anatomy per se, coexisting with severe atherosclerotic involvement that multiplies the likelihood of adverse events, as reflected in the outcome of the exercise testing, coronary angiography findings, and CT. Percutaneous treatment was feasible and effective in the short to medium term, pending longer follow-up.