The prognosis of patients with ST-segment elevation myocardial infarction (STEMI) has improved substantially in Spain over the past 20 years.1,2 This improvement has paralleled the expansion of reperfusion therapies and the progressive establishment of regional STEMI networks. With these advances, a large proportion of STEMI patients now benefit from percutaneous coronary intervention (PCI).1–3
The reduction in mortality achieved with fibrinolysis or primary PCI is crucially dependent on how soon these procedures are performed after diagnosis.4,5 One of the most effective ways to minimize time to reperfusion is for the health professionals making the first medical contact to decide on the therapeutic strategy and alert the catheterization laboratory, if appropriate, thus allowing treatment initiation in the in-hospital or out-of-hospital setting.6 This decision is almost always based on rapid interpretation of symptoms and the initial electrocardiogram (ECG), without waiting for the results of additional tests or consulting with other specialists. However, this policy carries a risk of imprecise diagnosis, especially compared with the ideal situation, albeit unachievable, in which all decisions would be taken by experts in STEMI patient care and ECG analysis and with access to any necessary complementary tests.
Imprecise diagnosis can be minimized through professional training and the implementation of clear and coordinated action protocols. STEMI networks also use an array of additional strategies, each of which has advantages and disadvantages; these strategies include automated ECG analysis, the inclusion of medical personnel or paramedics with ECG training in out-of-hospital emergency teams, and the digital transmission of the ECG to the coordinating center.3,6,7
Despite these measures, reported rates of false activation of the cardiac catheterization laboratory range from below 10% to almost 40%.7,8 This high variability is in part explained by the different criteria used to define catheterization laboratory false alarms. In some studies, but not in others, the definition includes instances where subsequent case review shows activation to have been inappropriate, independently of whether emergency coronary angiography was cancelled.7 Activation might be judged inappropriate because the clinical symptoms or electrocardiographic findings did not indicate the intervention or because of the presence of contraindications. Even when activation is appropriate, there is no consistent definition of a false-positive STEMI diagnosis. The most frequent definition is the absence of an identifiable culprit lesion on coronary angiography; however, there are other definitions, based on angiographic findings, myocardial necrosis markers, other tests, diagnosis at discharge, or combinations of these criteria (Table 1).
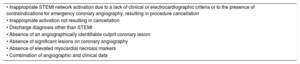
Criteria Used in Major Studies to Define STEMI Network False Alarms.7,8
| • Inappropriate STEMI network activation due to a lack of clinical or electrocardiographic criteria or to the presence of contraindications for emergency coronary angiography, resulting in procedure cancellation |
| • Inappropriate activation not resulting in cancellation |
| • Discharge diagnosis other than STEMI |
| • Absence of an angiographically identifiable culprit coronary lesion |
| • Absence of significant lesions on coronary angiography |
| • Absence of elevated myocardial necrosis markers |
| • Combination of angiographic and clinical data |
STEMI, ST-segment elevation myocardial infarction.
An efficient STEMI network would be one with the lowest possible number of inappropriate activations and an acceptable false-positive diagnosis rate among appropriately activated patients. Some authors have indicated an acceptable false-positive rate between 10% and 20%, based on data from angiography series.7,9 However, although there is abundant information available on the rates of false-positive activations in STEMI networks, less is known about the predictors of inappropriate activation and false-positive diagnosis.
In a recent article in Revista Española de Cardiología, Regueiro et al. reported the rates of inappropriate STEMI network activation and false-positive STEMI diagnosis among 5701 consecutive patients treated within the Catalonian STEMI network (Codi Infart) from January 2010 through December 2011.10 Inappropriate activations and false-positive diagnoses were identified according to angiographic or clinical criteria. Upon arrival of the patient at the primary PCI center, the attending cardiologists classified the STEMI network activation as inappropriate if the patient did not meet the established criteria: an electrocardiogram revealing a new ST-segment elevation or a new or presumed new left bundle branch block or clinical symptoms indicating a possible ischemic origin. False-positive STEMI diagnoses were defined angiographically as the absence of an identifiable culprit coronary artery or clinically as a discharge diagnosis other than STEMI.
Of the 5701 network activations, 87.8% were considered appropriate and 12.2% inappropriate. Approximately two-thirds of the inappropriate activations were due to the cardiologist at the primary PCI center disagreeing with the initial interpretation of the clinical symptoms, and the remaining third were related to differing interpretations of the ECG. The rate of inappropriate network activation showed no significant association with the place of activation, whether in a PCI-equipped hospital, a hospital without PCI capability, or an out-of-hospital emergency setting. Independent predictors of inappropriate network activation were advanced patient age, a history of myocardial infarction or left bundle branch block, and the presence of established complications. In-hospital mortality at 30 days was similar for patients with appropriate or inappropriate activation.
Among the 5007 patients with appropriate activations, a culprit artery was identified in 85.4%, with the remaining 14.6% having no identifiable causal lesion. Among the same patients, the discharge diagnosis was STEMI in 88.4% and an unrelated condition in 11.6%. The lowest rate of false-positive diagnosis was obtained when the STEMI code was activated by the emergency medical services, especially when activation was based on clinical criteria. The independent predictors of a false-positive diagnosis were female sex, a history of infarction or left bundle branch block, and–for the clinical definition–treatment at a hospital without PCI capability and the absence of major established complications. Most patients whose STEMI activation was judged to be a false positive were discharged with a diagnosis other than acute coronary syndrome. Adjusted short-term mortality was similar for patients with confirmed STEMI and those with a false-positive STEMI diagnosis.
The study provides a detailed analysis of the current prevalence of catheterization laboratory false alarms for STEMI in a large Spanish series. The study also makes a clear distinction between inappropriate network activation and false-positive diagnosis and defines false-positive diagnosis according to angiographic or clinical criteria. In addition, the study provides information on the predictors of inappropriate network activation and false-positive diagnosis and their influence on clinical outcomes. The authors are to be congratulated on the thoroughness of their analysis and clear presentation of the results, and commendations should be extended to all the professionals involved in the design, recording, and maintenance of the Codi Infart database, without whose efforts the study would not have been possible.
Some of the results deserve comment. The rate of inappropriate STEMI network activations is in line with previous findings7; nonetheless, the rate is relatively high, and efforts should be made to reduce it. Given the definition of inappropriate network activation (rejection of the initial diagnosis by the cardiologists at the receiving center), it is noteworthy that the rate of inappropriate activation was similar in PCI-equipped centers and other activation points, despite the presence in PCI-equipped centers of an on-call cardiologist. The report does not state the number of patients in whom activation was cancelled or whether classification as appropriate or inappropriate was possible after review of the coronary angiogram; this could have influenced the decision in borderline cases and could in part explain this contradiction. The study period (2010-2011) is soon after the Codi Infart launch, and it is thus possible that the rate of inappropriate activations has since decreased. This is especially likely in the out-of-hospital emergency setting, because emergency medical personnel have now had time to build expertise and confidence in decision making about patients with suspected STEMI. The association of inappropriate activation with a history of myocardial infarction highlights the difficulties of STEMI diagnosis in these patients. These difficulties are only partly overcome by comparing the ECG with older traces. STEMI diagnosis is even more difficult in the presence of left bundle branch block.11,12 In both situations, correct interpretation of symptoms is essential; however, when there is doubt, it is always better to risk an unnecessary activation than to ignore a possible STEMI and not activate the treatment protocol. Another concern is the association of inappropriate activations with the presence of established complications and the notable rate of PCI in this patient subgroup; this finding suggests that many of those affected are very high-risk NSTEACS patients requiring emergency coronary angiography.
The reported rate of appropriate network activations resulting in a false-positive STEMI diagnosis is also in line with previous studies.7,8 Unlike inappropriate activations, false-positive diagnoses showed a stronger association with patient-specific factors than with care protocols, and it may therefore be difficult to reduce their number. The lower false-positive diagnosis rate in the out-of-hospital setting suggests possible underlying differences between patients who alert the emergency services and those who arrive at hospital by their own means. A small proportion of false-positive diagnoses may result from thrombus lysis, since fibrinolysis was more frequently used in these patients. The higher prevalence of false-positive STEMI activations in women is in line with other female-specific STEMI features: a higher frequency of infarction in the absence of an obstructive coronary lesion,13 a distinct electrocardiographic presentation,14 and a higher prevalence of conditions easily confused with STEMI, such as tako-tsubo syndrome.15 False-positive STEMI diagnosis was also associated with a history of myocardial infarction or left bundle branch block. This finding might herald a future increase in the false-positive rate, in view of the recent recommendation for right bundle branch block to be included as an indication for STEMI activation on the same basis as left bundle branch block.9 Given the high false-positive rate in patients with a conduction defect on ECG, it would seem especially important to prioritize primary PCI above fibrinolysis in these patients unless the STEMI diagnosis is beyond doubt.
It would have been interesting if the article had identified the alternative diagnoses and causes of death among patients with false-positive STEMI activations, and the study would also have benefitted from some commentary on the associated economic impact. However, despite its limitations, most of which are mentioned in the original article, the study by Regueiro et al. illustrates the importance of an ongoing registry of patients entering STEMI networks as a tool for monitoring performance and designing measures for network improvement. The study also clearly confirms the benefit of coordinating all specialists and services involved in STEMI patient care in order to achieve the best possible outcomes.
FundingJ.A. Barrabés receives research funding from the Instituto de Salud Carlos III (PI16/00232) with cofunding from the European Regional Development Fund (ERDF).
Conflicts of interestJ.A. Barrabés has received payments from AstraZeneca and Menarini for educational activities.