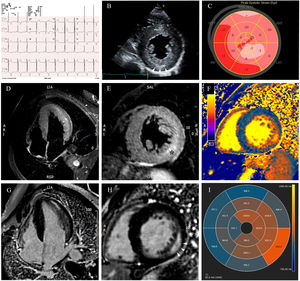

A 49-year-old man was referred to the emergency department for evaluation of atypical chest pain and palpitations. His electrocardiogram (figure 1A) was remarkable for short PR interval with signs of left ventricular hypertrophy. As troponin was slightly elevated, invasive angiography was performed, which was negative for coronary artery disease. A transthoracic echocardiogram (figure 1B, video 1 of the supplementary data) confirmed left ventricular hypertrophy with preserved ejection fraction, prominent papillary muscles, and increased inferolateral wall echogenicity (arrowheads). Deformation study revealed global longitudinal strain reduction (−13.2%), with regional involvement, mostly on epicardial layer assessment and circumferential strain analysis (figure 1C, video 1 of the supplementary data). Cardiac magnetic resonance (video 1 of the supplementary data) showed extensive edema (*) at both the lateral and inferolateral wall (figure 1D,E, STIR: short tau inversion recovery) with concomitant intramural late gadolinium enhancement (figure 1G,H, arrowheads). Myocardial mapping was noteworthy for abnormally low T1 values except for the lateral walls, where they were abnormally high (normal range: 972-1070ms) (figure 1F,I). This led to the hypothesis of Fabry disease, which was later confirmed from increased globotriaosylsphingosine (lyso-Gb3) serum levels and a pathogenic α-GalA mutation: c.902G>A, p.(Arg301Gln). Further investigation excluded renal and neurological involvement, angiokeratomas or visual impairment and identified 1 brother and 2 cousins with the disease (figure 2, family tree). Specific chaperone therapy with migalastat was proposed.


Despite the typical clinical and imaging findings supporting the diagnosis of Fabry cardiomyopathy, this case is notable for its specific tissular changes. Pseudonormalized and above normal T1 values, addressing changes such as inflammation and fibrosis, may follow distinct disease stages, eventually related to clinical events and troponin release. Regional function strain analysis matched tissue characterization.
Informed consent was obtained from this patient.
FUNDINGNot applicable.
AUTHORS’ CONTRIBUTIONSL. Oliveira wrote the first draft of this article. J. Abecasis and D. Brito incorporated feedback in subsequent revisions and reviewed the final draft. L. Oliveira composed the figure and video, which was also reviewed by J. Abecasis and D. Brito, and submitted the final version of this article on behalf of all the authors.
CONFLICTS OF INTERESTNone to declare.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.rec.2021.10.001