To the Editor,
The entrapment of a circular catheter in the mitral subvalvular apparatus is a rare but serious complication. We report here a case study about the maneuvers that can be performed to help release it as well as the frequent need for surgical treatment.
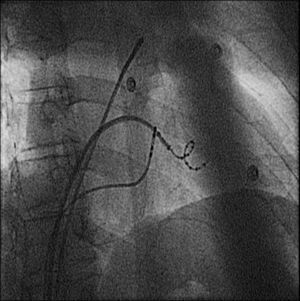
The subject is a 46-year-old male athlete with recurrent episodes symptomatic of paroxysmal atrial fibrillation (AF) despite antiarrhythmic therapy. An electrophysiological study was requested, to be performed using a transseptal approach with Mullins sheath and Brockenbrough needle (electrophysiological guide and single puncture). A 20-mm circular catheter (LassoNav®, Biosense Webster) and an irrigated-tip ablation cathether (Navistar®) were used. Using a non-fluoroscopic navigation system (CARTO V.10), an electroanatomic reconstruction of the left atrium and pulmonary veins (PV) was performed. After isolating both the left PV and the right superior PV, the 20-mm circular catheter was replaced by a low-caliber 15-mm catheter (LassoNav®, Biosense Webster) to access the inside of the right inferior PV. The catheter shifted into the left ventricle during placement and remained trapped in the subvalvular apparatus. An unsuccessful attempt was made to free it by gently advancing the catheter with a clockwise rotation and traction on the catheter, with and without the support of the Mullins sheath, which was advanced to the distal end of the catheter in an effort to straighten it. These maneuvers were repeated, without success, during ventricular pacing at 220 bpm to reduce cardiac output during adenosine-induced asystole, and under Isoproterenol infusion administered to increase inotropism. A 4-mm ablation catheter with a deflectable distal tip was introduced by a retrograde approach to surround the distal end of the multipolar guide and modify the traction point, like a “lasso” catheter to encircle the distal tip of the circular catheter. However, this too failed to release it. The fluoroscopic view of the circular tip of the catheter made us suspect a fracture of the distal portion (Figure 1), and given the high risk of valvular lesion, as reported in similar cases, we decided to terminate the procedure and proceed with surgical extraction. The mitral valve was accessed through median sternotomy and transverse aortotomy while under cardiopulmonary bypass. During the procedure, a transesophageal echocardiogram was performed that showed grade II/IV mitral regurgitation (MR) and trapping of the circular portion of the catheter between the chordae of the anterior mitral leaflet. It was not possible to release it using traction during surgery, and it became necessary to section the circular portion into three parts. Despite immediate postoperative AF, the patient had a favorable evolution. The echocardiogram prior to discharge showed trivial MR that had already been reported in the pre-ablation study.

Figure 1. Catheter trapped in the mitral subvalvular apparatus.
Very few cases of circular catheter entrapment in the mitral valve apparatus have been published and most have been produced using catheters with diameters of between 10 and 20mm (more commonly 10, 12 or 15mm). Some have been freed by advancing the sheath over the catheter and rotating it clockwise around the catheter.1 There have been reports of breakage in the circular portion of the catheter and percutaneous extraction2 while performing these maneuvers, although most have required surgical intervention due to failure of extraction attempts or development of acute MR due to rupture of the subvalvular apparatus or commissural tearing.1,2 There are also reports of catheter release and extraction using minimally invasive surgery.3
This complication is rare but probably also underestimated. In a recent record of 8745 patients that underwent AF ablation, only one case of unspecified valvular damage was reported.4 However, a retrospective review of 348 patients found that the incidence of circular catheter entrapment in the mitral valve apparatus was significantly higher (0.9%).1
There are no reports on the usefulness of maneuvers designed to reduce cardiac output or increase contractility in an effort to facilitate the release of the catheter, but in our case they were not effective.
The published data indicate the need to consider the risk of injury to the mitral valve and to rely mainly on the maneuver of advancing the sheath over the catheter using clockwise rotation, resorting to surgical extraction if this maneuver is not effective.
Corresponding author: irene.valverde.andre@gmail.com