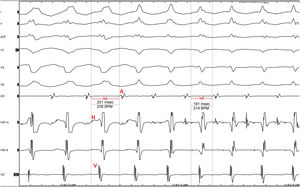
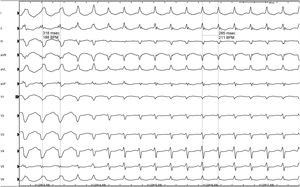
A 56-year-old patient with no relevant history attended the emergency room because of an episode of rapid palpitations. An electrocardiogram showed regular broad QRS tachycardia at 190 bpm, with a similar morphology to left bundle branch block. In view of the good clinical and hemodynamic tolerance, a 6 mg bolus of adenosine was administered, and the patient entered stable sinus rhythm with narrow QRS and no signs of pre-excitation. Echocardiography ruled out structural heart disease and the patient was referred for electrophysiological study. Measurement of baseline intervals produced normal results. Initial catheter manipulation induced the tachycardia shown in figure 1, superimposed on the clinical tachycardia, and QRS narrowing was observed with a change in morphology as well as transient acceleration.

In view of the ECG (figure 1) and the intracavitary ECG of the episode (figure 2), what was the most likely diagnosis?
- 1.
Ventricular tachycardia of the right ventricular outflow tract
- 2.
Atrial tachycardia with bundle branch aberration
- 3.
Orthodromic atrioventricular re-entrant tachycardia
- 4.
Intranodal re-entrant tachycardia

Submit your answer to http://www.revespcardiol.org/en/electroreto/73/07. The solution will be published in the next issue (August 2020). #ECGChallenge.