To the Editor,
Coronary artery fistulas are a rare congenital coronary anomaly. Although often small and diagnosed by chance, they can cause a wide range of symptoms associated with myocardial ischemia, including sudden death.1
We present the case of a 63-year-old woman with cardiovascular risk factors of overweight, smoking, and high blood pressure. For several years, following moderate effort the patient had reported symptoms clearly indicating angina although these had always been labeled as of musculoskeletal origin. She came to the Emergency Room following a more prolonged episode than normal that occurred while resting and after a family argument. The electrocardiogram showed no changes, and serial measurements of cardiac enzymes and baseline echocardiography were normal. Exercise testing performed 1 day later was inconclusive, with mild clinical symptoms of angina at the start of Bruce protocol stage 3, without reaching maximum heart rate (MHR). Leads V5-V6 did show a slight but nonsignificant tendency towards ST-segment depression. Given these results, the patient underwent dobutamine stress echocardiography. On reaching 135 bpm, she presented the same symptoms of angina accompanied by ST-segment depression in precordial leads V4-V5, I, and aVL, as well as akinesia in all apical and mid-inferior segments. The test was interrupted and analytical tests 6h later revealed a 0.25 ng/ml troponin T peak.
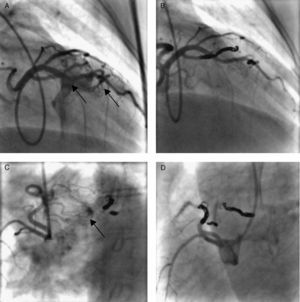
Coronary angiography showed the absence of significant atherosclerotic lesions. From the left anterior descending artery proximal and mid segments, a dual coronary artery fistula drained into the right ventricle (Figure 1A). The underdeveloped right descending coronary artery presented another coronary artery fistula draining into the right ventricle (Figure 1C). Both fistula paths were occluded by deploying 10 coils via radial access (Figure 1B and D). Final results were good with no complications.

Figure 1. A: dual coronary artery fistula in left anterior descending artery draining towards the right ventricle. B and D: closure of both fistula paths by coil implantation. C: fistula in right descending coronary artery also draining into the right ventricle.
During her check-up after 8 weeks, the patient reported a clear improvement in functional class, having presented no further symptoms of angina despite receiving no anti-angina drugs other than 100mg losartan/day for high blood pressure control for more than 6 years. She underwent control exercise testing, completing the Bruce protocol stage 3 and reaching 96% of MHR with neither electrical nor clinical changes. During a second stress echocardiograph test, she reached MHR in the maximum stage of 40μg/kg/min without presenting electrical or echocardiographic changes.
A congenital coronary artery fistula is an abnormal communication between an epicardial coronary artery and a cardiac chamber or vascular structure located near the heart: 40% to the right ventricle, 25% right atrium, 15% to 20% pulmonary artery and 7% coronary sinus.1 It is found in approximately 0.10% to 0.15% of coronary angiographies and most frequently affects the right descending coronary artery (60%).1, 2, 3 It is usually found by chance with no identifiable associated symptoms, but symptoms do appear when the shunt is significant, fundamentally variable degrees of ischemia and of heart failure.2
Dual coronary artery fistulas affecting both coronary territories are extremely rare (5% of the total) and more frequently present phenomena of secondary coronary ischemia than of significant left-right shunt with phenomena of “coronary steal”.4 The percutaneous approach and coil deployment–which is less invasive and involves a shorter hospital stay–is the current method of choice.2 In our case, it permitted symptom control with proven absence of inducible ischemia in the follow-up. Surgical closure is currently reserved for large multiple fistulas, which are generally diagnosed in childhood,2 when different technical considerations need to be borne in mind.3
Corresponding author: niemed21@hotmail.com