To the Editor,
Idiopathic ventricular fibrillation (VF) is responsible for approximately 8% of the cases of sudden cardiac death, and occult channel defects have been reported to be among the possible causes.1 On rare occasions, it is triggered by an electrical storm, in which case catheter ablation is the only alternative when drug therapy fails.2
We present the case of a 53-year-old woman with nothing remarkable in her medical history, who had been asymptomatic until she was admitted to the hospital with a syncopal episode. Monitoring demonstrated the presence of polymorphic ventricular tachycardia with spontaneous cessation and frequent monomorphic premature ventricular contractions (PVC), with left bundle branch block and left superior axis morphology and a short coupling interval that triggered repeated episodes of VF, requiring defibrillations on 20 occasions over a period of 72h.
The baseline electrocardiogram was normal. Metabolic disorders, toxic substance intake and structural heart disease were ruled out by means of echocardiography, coronary angiography, cardiac magnetic resonance imaging, and the determination of adrenaline and flecainide concentrations.
A first electrophysiology study (EPS) was carried out as an emergency measure because the frequent recurrences of VF persisted despite amiodarone infusion, requiring defibrillations. The last episode occurred during transfer to the electrophysiology laboratory where, after introduction of catheters into the His bundle and the apex of the right ventricle (RV), neither PVC nor other arrhythmias developed.
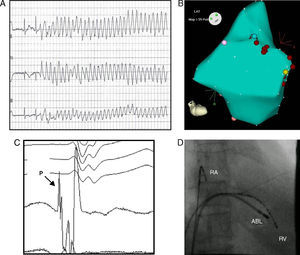
Four hours after completion of the EPS, the VF-inducing PVC reappeared, requiring further defibrillations that were not prevented by the infusion of isoprenaline, beta blockers, or procainamide; for this reason, the EPS was repeated the next day. From mid septum to apical septum of the RV, Purkinje potentials were recorded in relation to the distal insertion of the right branch, potentials that preceded the initiation of the QRS of the self-limiting VF-inducing PVC by 45ms on one occasion (Figure 1). Applications of radiofrequency suppressed the PVC and the episodes of VF. Seven days later, a single-chamber automatic defibrillator was implanted and, after 10 months of drug-free follow-up, the device has recorded no ventricular arrhythmias. The genetic study detected a novel frame-shift mutation in the sodium channel alpha subunit gene SCN5A (D1816fs), which results in early transcriptional arrest and produces a truncated or shortened protein.

Figure 1. A: electrocardiographic tracing at hospital admission with an episode of ventricular fibrillation initiated by premature ventricular contraction. B: electroanatomic mapping of right ventricle, using the CARTO® system, in which no low voltage zones were observed. The sites to which radiofrequency energy was applied are indicated in red. C: right oblique fluoroscopic view showing catheters in right atrium and right ventricular apex and ablation in apical septum. D: Purkinje potential at the site of the origin of the premature ventricular contractions. ABL, ablation; RA, right atrium; RV, right ventricle; P, Purkinje potential.
The major mechanism of sudden cardiac death is VF and the most common cause is ischemic heart disease. Ventricular fibrillation is considered to be idiopathic when there is no evidence of structural heart disease, cardiotoxicity, electrolyte disorders, or a predisposing hereditary condition.1
Although PVC is a benign arrhythmia, there are cases in which PVC originating in the Purkinje system or in the RV outflow tract initiates VF episodes in individuals without heart disease, with structural heart disease, or with channel defects. The absence of heart disease and the early development of PVC fit well with the entity described by Leenhardt et al.3 Haïssaguerre et al reported the efficacy of radiofrequency ablation in PVC in the prevention of new episodes of VF over the short and long terms.2
This case is singular for 2 reasons. On one hand, it highlights the efficacy of ablation in this desperate situation and the difficulty derived from the mechanical suppression of the focus via catheter. On the other hand, it describes a novel mutation in the SCN5A gene as a cause of idiopathic VF with a normal electrocardiogram. Thus, it involves an occult channel defect of which VF was the first sign. The incomplete penetration of channel defects explains the fact that individuals with FV who have an apparently normal heart and in whom there is no electrocardiographic evidence of this condition exhibit electrical instability in relation to a genetically determined occult arrhythmogenic disease.1
Corresponding author: luis.tercedor.sspa@juntadeandalucia.es