Coronary angiography is the gold standard for the study of coronary artery disease. This technique requires several orthogonal projections. Rotational angiography is a new technique which involves pre-set rotation of the X-ray tube around the patient and allows visualization of each coronary artery in different views, using a single contrast injection. The purpose of this study was to compare conventional coronary angiography (A) vs rotational angiography (B), focusing on radiation dose, amount of contrast administered, and total procedure time for both diagnostic and therapeutic percutaneous coronary interventions.
MethodsProspective study of 104 consecutive patients undergoing coronary angiography who were randomized to one of these techniques.
ResultsWe found a significant reduction in the amount of contrast administered (A vs B, 93.1 [41.7] vs 50.9 [14.7] mL; P<.0001) and radiation exposure (27.6 [11.5] vs 18 [6.4] mGycm; P<.0001). A significant increase in total procedure time was noted in the rotational angiography arm. However, when only the last 50 patients were analyzed, we found no difference in procedure time between the groups, probably related to the learning curve of the operators. Angioplasty was performed in 29 patients in group A and 28 patients in group B. Contrast reduction was maintained in the rotational angiography group compared to the conventional technique (A vs B, 335.1 [192.1] vs 238.5 [114.4] mL; P=.02).
ConclusionsThe rotational angiography technique leads to a significant decrease in radiation exposure and contrast dose administered for diagnostic procedures when compared to conventional coronary angiography. In patients who undergo percutaneous coronary intervention, contrast reduction remains significant.
Keywords
.
IntroductionCoronary angiography is the gold standard for the study of coronary artery disease. The conventional technique requires standard orthogonal views, with at least 3 to 4 views for the left coronary artery and 2 for the right.
Nevertheless, assessment using fixed 2-dimensional views of a 3-dimensional structure has major inherent limitations.1 The safety and efficacy of conventional angiography depend on the operator's learning curve, decision-making skills, and expertise in determining the best views for optimal treatment of patients. A lack of skill usually leads to coronary studies with higher amounts of contrast medium and radiation doses.2, 3
The contrast volume, the direct relationship with contrast-induced nephropathy, and the impact on the prognosis of patients who undergo percutaneous coronary intervention make it highly desirable to develop improvements in the techniques that would reduce contrast amount and the incidence of nephropathy.4, 5, 6, 7, 8, 9
Exposure to ionizing radiation from medical images can be harmful. Ionizing radiation can cause chromosomal changes, and at high doses is associated with an increase in the probability of malignant tumor; therefore, it is highly desirable to minimize the radiation dose during each procedure for both the patient and the operator.10, 11
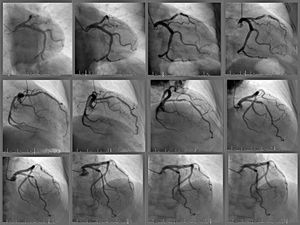
In this context, rotational angiography was developed: initially, as single-axis rotational angiography to allow 120° or 180° independent cranial and caudal rotational (left-to-right) movement,12, 13, 14, 15, 16, 17 and eventually, as XPERSWING rotational angiography for dual-axis rotational (cranial-to-caudal and left-to-right) movement to study the left and right coronary arteries with a single contrast injection for each artery. This rotational X-ray tube motion allows continual acquisition of both routine conventional angiography views and all intermediate views, thus permitting optimal assessment of the diseased segment that will be treated (Figure 1).1, 18, 19

Figure 1. Acquisition sequence of rotational angiography. From left to right, and from top to bottom: left caudal, right caudal, right anterior oblique, right cranial, cranial, and left cranial. Note the lesion in the middle segment of the anterior descending artery.
Our purpose was to compare rotational angiography with the conventional technique in routine practice.
Methods ObjectivesThe main objective was to determine if coronary artery disease can be investigated with reduced contrast volume by rotational angiography, compared to the conventional technique in routine practice; a more specific objective was to determine the contrast volume (mL) administered to patients who undergo diagnostic coronary angiography with rotational technique compared to the conventional technique. Additional objectives of the study were to determine the contrast volume (mL) administered to patients who undergo angioplasty in both groups, to determine the total radiation dose from the dose-area product (DAP) (mGycm2) and cumulative air Kerma (mGy) in both groups, and to determine procedure time and fluoroscopy duration (min) in both groups.
Study PopulationThe inclusion criteria for the study were age >18 years, referral for elective coronary angiography, and signed informed consent.
The study excluded any patients who had been referred for elective angioplasty, had a history of coronary revascularization surgery, dialysis, ST-elevation infarction within the previous 24 h, or cardiogenic shock, or were unable to give consent.
Study DesignThe study was designed as a prospective, randomized, nonblinded experimental study and was approved by the respective ethics committee at our hospital.
We estimated the sample size based on data published on contrast amounts administered with rotational angiography compared to the conventional technique.15, 16, 17, 18, 19 The study required 46 patients in each group to detect a difference ≥20 mL in contrast medium, assuming an alpha risk of .05, a beta risk of .05 in a 2-tailed hypothesis test, and a common standard deviation of 25 mL of contrast medium in both groups. According to these data, a total sample size of 92 patients was required. Assuming 10% losses and because patients are readily recruited, we decided to include 110 patients (55 in each group). Patients who met the inclusion and exclusion criteria after signing the informed consent were randomized by a random number table to conventional angiography or rotational angiography.
Conventional angiography was performed with at least 3 views of the left coronary and 2 of the right coronary. The number of views obtained was decided by the operator, but were sufficient to characterize the lesion adequately, in the event that angioplasty was necessary. The contrast amount used in conventional angiography in each injection was 8 to 10 mL at 4 mL/s for the left coronary and 6 mL at 3 mL/s for the right coronary.
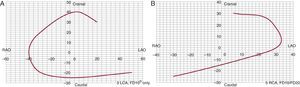
Following catheter placement, rotational angiography requires finding the isocenter (neutral position that allows continuous acquisition by rotating that tube around the patient), by first centering over the patient's height, in left lateral view, and subsequently in the anteroposterior view at 0°. The isocenter was determined for the left and right coronary arteries. A single contrast injection of 14 mL at 2.5 mL/s was given for the left coronary and 10 mL at 2 mL/s for the right coronary. A 40°, 5.8-s left coronary artery cranial swing was used for the left coronary, and a 4.0-s anteroposterior right coronary artery swing was used for the right coronary. Figure 2 shows the detector trajectory during acquisition in both coronaries.

Figure 2. Detector trajectory with the XPERSWING technique. A, left coronary. B, right coronary. LAO, left anterior oblique; LCA, left coronary artery; RAO, right anterior oblique; RCA: right coronary artery.
The diagnostic or therapeutic catheter was chosen by the operator.
In all cases, an ACIST CVi® (ACIST Medical Systems, Eden Prairie, Minnesota, United States). automatic contrast injector was used. The contrast amount displayed on the injector at the end of each procedure was recorded as the amount administered, whereas the radiation dose was obtained from the automatic analysis performed by the equipment. In both groups, the same exposure mode (low quality, fluoroscopy at 7.5 images/s, and cine acquisition of 15 images/s) was used. The contrast amounts and radiation were measured at the end of the diagnostic study, as well as at the end of the therapeutic procedure in patients who underwent interventional cardiology procedures.
Ventriculography, if necessary, was performed at the end of the diagnostic study and was excluded from the analysis of contrast amount and radiation.
The procedure time began to be measured when the first coronary being studied was visualized, using a timer set by the same operator on the Allura FD10® touchscreen, until the end of the diagnostic procedure, thus including the isocenter location time for both coronaries.
All studies were performed using the same equipment (Philips FD10® Digital X-Ray system, Philips Healthcare, Best, The Netherlands).
Statistical AnalysisThe qualitative variables are expressed as percentages, and were analyzed by the χ2 and exact Fisher tests. The quantitative variables are expressed as mean (standard deviation) or median (range). We first checked the sample distribution by the Kolmogorov-Smirnov test, using the Student t test (normal distribution) or nonparametric Wilcoxon and Mann-Whitney tests (non-normal distribution) for the analysis. SPSS version 15 was used for the statistical analysis.
ResultsA total of 110 patients were randomized between February and April 2009; 6 patients were excluded from the study (2 for catheter instability, 1 for pressure drop caused by coronary trunk lesion, and 1 for independent outflow from the anterior descending and circumflex arteries). A total of 104 patients (52, conventional angiography; 52, rotational angiography) were analyzed.
The patient characteristics are shown in Table 1. There were no differences in baseline characteristics between the groups. A right radial approach was used in virtually all patients in both groups, except for 2 patients (1 left radial; 1 right femoral), both of them in the rotational angiography group.
Table 1. Baseline Patient Characteristics
| Group A | Group B | P | |
| Male sex | 36 (69.2) | 36 (69.2) | 1 |
| Age, years | 67±11 | 64±11 | .19 |
| Weight, kg | 80.2±14.3 | 77.5±10.8 | .27 |
| Height, cm | 165.4± 9.6 | 162.2±22.3 | .34 |
| Hypertension | 36 (69.2) | 34 (65.4) | .83 |
| Diabetes mellitus | 22 (42.3) | 14 (26.9) | .14 |
| PVD | 6 (11.5) | 2 (3.8) | .26 |
| LVEF | 50.48±14.90 | 53.30±1.90 | .47 |
| Previous PTCA | 16 (30.8) | 14 (26.9) | .82 |
| Hemoglobin, g/dL | 12.9 ±1.8 | 13.4± 1.8 | .19 |
| Creatinine, mg/dL | 1±0.3 | 0.9±0.2 | .16 |
| Indications | .15 | ||
| Chest pain study | 3 (5.8) | 7 (13.5) | |
| Stable angina | 15 (28.8) | 14 (26.9) | |
| Unstable angina | 18 (34.6) | 17 (32.7) | |
| NSTEMI | 8 (15.4) | 13 (25) | |
| STEMI >24 h | 8 (15.4) | 1 (1.9) | |
| Right radial access | 52 (100) | 50 (96.2) | .17 |
| Catheter diameter | .71 | ||
| 5 Fr | 49 (94.2) | 47 (90.5) | |
| 4 Fr | 3 (5.8) | 5 (9.6) | |
| Coronary artery disease, LCT | 7.1 (2) | 3.4 (1) | .66 |
| Coronary artery disease, AD | 55.2 (16) | 75 (21) | .16 |
| Coronary artery disease, Cx | 11 (37.9) | 9 (32.1) | .78 |
| Coronary artery disease, RCA | 14 (48.3) | 14 (50) | 1 |
| Multivessel | 10 (34.5) | 12 (42.9) | .59 |
| Complete revascularization | 22 (75.9) | 17 (60.7) | .26 |
AD, anterior descending artery; Cx, circumflex artery; group A, conventional angiography; group B, XPERSWING dual-axis rotational angiography; LCT, left coronary trunk; LVEF, left ventricular ejection fraction; NSTEMI, non-ST-elevation myocardial infarction; PTCA, percutaneous transluminal coronary angioplasty; PVD, peripheral vascular disease; RCA, right coronary artery; STEMI, ST-elevation myocardial infarction.
Values are expressed as no. (%) or mean ± standard deviation.
The diagnostic study was performed using 5-Fr diagnostic catheters in more than 90% of the patients in both groups and the 4-Fr in the remainder. 6-Fr catheters were not used in any patients for the diagnostic study (Table 1).
The mean number of conventional angiography views was 6.08, compared to 2.2 in the XPERSWING group; 5 patients required additional views to those obtained by rotational angiography: in 2 cases to assess collateral heterocoronary circulation in patients with chronic occlusions, in 2 cases for technique failure (inadequate contrast medium in the coronary vasculature), and in 1 case to optimize acquisition for assessment of a distal trunk lesion. The view repeated most often (4 patients) was a cranial view with noticeable right angulation. No diagnoses previously made by rotational angiography were changed by the results of the additional views.
Ventriculography in the diagnostic studies was excluded from the analysis, and none of the patients who underwent interventional cardiology required it. No adverse effects (decreased blood pressure or arrhythmias) associated with prolonged coronary injections were observed in any patients.
Contrast VolumeThe contrast volume used in the diagnostic procedure was significantly lower in the rotational angiography group, with a reduction of up to 46% (Table 2).
Table 2. Diagnostic Results
| Conventional Angiography | XPERSWING | P | |
| Diagnostic coronary angiography | |||
| Patients | 52 | 52 | |
| Contrast volume, mL | 93.1 (41.7) | 50.9 (14.7) | <.0001 |
| DAP, mGycm2 | 27.6 (11.5) | 18 (6.4) | <.0001 |
| Kerma, mGy | 458.8 (184.8) | 210.7 (83.9) | <.0001 |
| Fluoroscopy duration, min | 3 (2.1) | 3.1 (1.6) | .72 |
| Procedure time, min | 5.5 (2.4) | 6.5 (2.5) | .02 |
| Procedure time, last 50 patients, min | 5 (2.1) | 5.5 (2.4) | .19 |
| Diagnostic and therapeutic coronary angiography (total) | |||
| Patients | 29 | 28 | |
| Total contrast volume, mL | 335.1 (192.1) | 238.5 (114.4) | .02 |
| Total DAP, mGycm2 | 110.01 (90.78) | 90.20 (63.90) | .34 |
| Total Kerma, mGy | 1860.3 (1473.8) | 1277.8 (864.9) | .07 |
DAP, dose-area product.
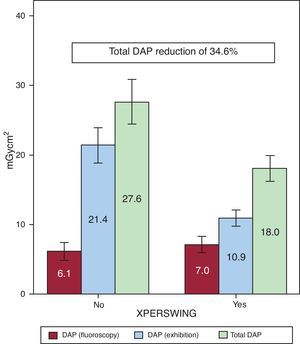
The radiation dose (DAP and Kerma) during the diagnostic procedure was significantly lower in the rotational angiography group, with a decrease of almost 35% compared to the dose administered during cine exposure (exposure DAP) (Figure 3).

Figure 3. The XperSwing group showed a mean decrease of 34.6% in radiation dose, as measured by the dose-area product, compared to the conventional technique. The dose reduction was mainly due to the dose-area product (exposure). DAP, dose-area product.
No significant differences in fluoroscopy duration were observed between the groups, but there were differences in procedure time, which was somewhat longer in the rotational angiography group (5.5 [2.4] vs 6.5 [2.5] min; P=.02). An analysis of the procedure time for the last 50 patients enrolled in the study showed disappearance of the difference (5 [1.3] vs 5.5 [1.2] min; P=.16), which was present in the first 50 patients (6.1 [2.1] vs 7.5 [3.1] min.; P=.01) (Table 2).
Therapeutic ProcedureA coronary interventional procedure was performed in 29 patients of the conventional angiography group and 28 in the rotational angiography group. There were no significant differences in procedure characteristics between the groups (Table 1). A significant reduction of 29% in total volume of contrast medium used (diagnostic and therapeutic procedure) occurred in the rotational angiography group, but there were no differences in radiation dose (Table 2).
DiscussionSeveral studies have compared rotational angiography as an effective technique for the diagnosis of coronary disease, showing that it is not inferior to the conventional technique and is even superior in certain segments (first diagonal, distal right coronary, posterior descending, and posterolateral trunk) but inferior in very calcified coronaries, collateral circulation, and TIMI flow.15 Klein et al.18 studied 30 patients by conventional angiography, followed by rotational angiography (XPERSWING). Two independent operators analyzed the number of lesions >50% with both techniques, and found a close correlation and absence of significant differences between them. Quantitative angiographic analysis was not used, and the study was performed with 6-Fr catheters. Our series is the largest dual-axis rotational angiography study currently published. Previous studies consistently found a significant decrease (19%-61%) in contrast amount and radiation dose,15, 16, 17, 18, 19 except in an early single-axis rotational angiography series published by Akhtar et al.,14 (2005) due to the different protocols applied and the development of the X-ray systems used.14
Our study observed a significant decrease in total radiation dose, with no differences in fluoroscopy time. Unlike the conventional technique, in the rotational technique more time is spent on fluoroscopy to locate the isocenter and less time on cine acquisition (Figure 3).
In our series, rotational angiography usually involved a slight increase in procedure time. The published studies consistently report no increase, and a decrease was observed in the most recent series published.18 All studies underscore the importance of the learning curve, and this is confirmed among the last 50 cases in our series, which showed no significant differences in procedure time. In fact, the learning curve is important for both the operators and other medical staff, and in siting patient-related devices (intravenous medication) to prevent collisions that could slow the procedure.
Prolonged coronary injection may be related to arrhythmic events and drops in blood pressure. Its safety has recently been analyzed, and no significant clinical changes in heart rate or blood pressure have been observed in injections of up to 7.2s.13 This safety was confirmed in later studies.18 Although the endpoints of our series did not include adverse effects (arrhythmic events or drop in blood pressure) related to prolonged injections no longer than <7.2s, none of the patients experienced any such event.
In our opinion, this study revealed an important difference compared to previous studies, in the sense that it more closely reflects the usefulness of the technique in routine practice. In all published studies, femoral access and 6-Fr diagnostic catheters were used.14, 15, 17, 18 Our series did not distinguish between any kind of access, although our results are applicable to the right radial access, given that virtually all procedures were performed using this approach, solving, with an appropriate learning curve, the problems of collision involved in holding the arm and remaining in close proximity to the X-ray tube. There were no differences between the two techniques in terms of the first and second operator's location inside the catheterization lab. More than 90% of procedures were performed with 5-Fr diagnostic catheters, with 4-Fr catheters used in the others. We found no differences in procedure success between the 5-Fr and 4-Fr catheters; however, because of the limited used of 4-Fr catheters, no conclusions on routine use can be drawn. This finding is of interest, as the radial approach and 5-Fr diagnostic catheters are increasingly used in routine practice.
The procedure time and contrast amount were analyzed as a whole, rather than independently in the study of each coronary, as currently reported.13, 14, 15, 17, 18 Thus, our analysis included the contrast used in catheter exchange and during catheter placement in the coronary arteries. All contrast administered to the patient is important and, therefore, the aim was to conduct a real-life study of how much contrast is used in a rotational angiography procedure.
Not all patients require the same number of views to characterize the coronary anatomy adequately. Rotational angiography is standard for all patients, providing the most information with a highly stable amount of contrast medium. This is the first study to analyze the contribution of the technique to patients who undergo coronary interventional procedures. There were no differences in the amount of radiation, but the savings in contrast administered in the XPERSWING group was maintained, with a decrease of 29% compared to the conventional technique. A mean difference of 42 mL in the diagnosis increases the total average difference to 96 mL when coronary interventional procedures are performed. We have no clear conclusions on why this occurs, but we believe that it may be related to 2 concepts: a) the ideal reference view, and b) the amount of contrast medium needed to obtain it. Rotational angiography provides more information when the coronary disease is more severe and the anatomy is more complex, because a single injection of contrast medium allows standard views and all intermediate views to be obtained, which allows the lesion to be characterized more accurately and the reference view to be obtained with a small amount of contrast medium, thus ensuring a faster and safer angioplasty.
We would like to conclude by paraphrasing Schwartz20 in his editorial: “We are on the way toward finding safer, more rapid ways to perform invasive study of coronary disease and laying the ground for new clinical applications.”
Study LimitationsThe contrast amount per coronary injection was 8 to 10 mL for the left coronary and 6 mL for the right, as this is routine practice in our setting. If smaller amounts of contrast medium in each injection are defined in the protocol for conventional angiography, it could probably decrease the differences observed between both techniques in contrast amount.
A fundamental limitation of our study was that imaging quality and diagnostic capacity were not objectively assessed by comparing both techniques. Further studies should investigate this aspect of the technique.
The incidence of contrast-induced nephropathy was also not analyzed, although a decrease in contrast amount is one of the first steps to help lower the incidence.5, 7
No skin dosimeters were used by the patients or operators, and dosimetric data were only available from the equipment itself. The implications of this decrease in radiation should be determined for patients and for operators continuously exposed to the radiation source.
Patients in poor condition (cardiogenic shock, ST-elevation acute myocardial infarction less than 24 h earlier) were excluded. Nevertheless, these patients would probably benefit most from careful techniques and procedures using minimal amounts of contrast medium.
ConclusionsDual-axis rotational angiography (XperSwing) allows coronary disease to be investigated with the same efficacy and with greater patient safety by achieving a significant reduction in the contrast volume administered and the radiation dose.
In the diagnosis of coronary disease, rotational angiography uses less contrast medium than the conventional technique in patients who undergo a coronary interventional procedure.
An adequate learning curve will prevent any increase in study duration, compared to the conventional technique.
Conflicts of interestNone declared.
Received 7 September 2011
Accepted 7 December 2011
Corresponding author: Alfonso XII 19, 3.o A, 21003 Huelva, Spain. aegmenchero@hotmail.com