To the Editor:
We report the case of an unusual, but nevertheless severe, complication associated with entrapment of a catheter during a procedure for percutaneous ablation.
The patient was a 30-year-old man with Wolff-Parkinson-White (WPW) syndrome (inferoseptal pathway). After attempting unsuccessful venous radiofrequency ablation with a conventional irrigated-tip catheter, a second retrograde aortic arterial approach was made with a Medtronic-MarinrMCTM catheter.
During mapping with the usual maneuvers in the left atrioventricular sulcus, the catheter was noted to be entrapped in the mitral subvalvular apparatus. An emergency echocardiogram confirmed the entrapment of the tip and mitral regurgitation when the catheter was pulled. Several different maneuvers were used in an attempt to free the catheter, including clockwise and anti-clockwise twisting, gentle advances and traction, as well as combinations of these maneuvers, followed by the use of various catheters advanced to the tip and used as a sheath, but without managing to release the catheter.
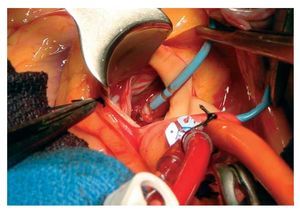
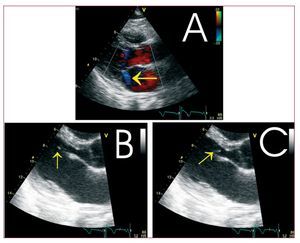
In view of the risk of damage to the mitral apparatus with the use of more aggressive percutaneous techniques, it was decided to release the catheter by means of surgery, employing extracorporeal circulation and transverse aortotomy. During the surgery, the last few millimeters of the catheter were seen to be entrapped by four chordae tendineae of the anterior leaflet that were rolled up in it (Figure 1) and rupture of a secondary chord. The catheter was released and visual inspection showed no abnormalities. An echocardiogram 6 days later showed rupture-elongation of the secondary chord with mild mitral regurgitation (regurgitant area of 1.8 cm2), with no repercussion to the left ventricle (Figure 2).

Figure 1. Intraoperative image of the twisted chordae tendineae entrapping the tip of the radiofrequency catheter.

Figure 2. Postsurgical echocardiogram (parasternal long axis) showing: A: absence of prolapse of the anterior leaflet with mild mitral valve regurgitation seen with color Doppler (arrow). B and C: mobile echocardiogram of the ruptured chord at 2 moments of diastole (arrows).
Venous access in inferoseptal accessory pathways using radiofrequency in the tricuspid annulus or the coronary venous system is often ineffective, with a greater rate of second procedures because a left-sided approach is necessary. The retrograde aortic approach to the mitral annulus enables risks derived from transseptal puncture to be avoided, with similar rates of success.
The anatomical complexity of the mitral subvalvular apparatus quite often leads to varying degrees of catheter entrapment, whether noticed or not, although they can generally be released by such maneuvers as rotating, traction or forward advancement. However, minor valve damage as a result of these maneuvers is not exceptional, with a reported incidence in the aortic retrograde approach of 1.9%-9%, with mitral regurgitation (1.1%-9%) being more common than aortic regurgitation (1.1%-3.4%).1-3 Aortic valve damage requiring emergency surgery has also been described during procedures for catheter ablation, and severe mitral valve damage that required surgical intervention up to several months after the procedure. Follow-up of minor valve lesions has shown no progression of the lesion, and prophylaxis against infectious endocarditis is recommended.1,2
The prospective Atakr registry, using the same technology as in our case, found an incidence of major valve damage of 0.1%.3 The NASPE Survey on Catheter Ablation reported incidences of 0.07% for the aortic valve and 0.04% for the mitral valve, with 1 case requiring surgery due to entrapment of the catheter that was "lodged in a trabeculae around the mitral valve."4 No cases have yet been reported in the Spanish registry.5
Two cases have been published of catheter entrapment in the left WPW syndrome6,7; one was cleared percutaneously and the other after cardiac surgery. It is noted that the incidence of this complication may be underestimated, considering the voluntary character of the registries and reports to the manufacturing companies, which themselves estimate an incidence of 0.017%.7The current expansion of procedures using the left approach, and occasionally with different catheters with a circular tip placed in the left atrium, could lead to an increase in the frequency of this complication.8,9 An incidence of atrial fibrillation during ablation procedures of 0.9% (0.2%-2.5%) has already been reported.10 However, no predisposing factors for its appearance have yet been identified.
Reports exist of release of the entrapped catheter tip by means of a guide catheter being used as a sheath that was advanced to the tip, to straighten it and thus provide tension.9,10 It has been suggested that for circular catheters entrapped during the transseptal approach, advancement of the catheter with clockwise rotation might be more effective than simple rotation or pulling.9,10 The use of another "deflectable" catheter to apply pressure to the tip may be useful in certain cases.9 In the event of failure of gentle percutaneous maneuvers, release by surgical means has been proposed to be preferible.8,10
The present case provides an illustration of a complication that, although unusual, should nevertheless be taken into consideration.