A 69-year-old man with a history of aortic valve disease received an aortic valve replacement in 1996. He was reoperated on 5 occasions for prosthetic valve dysfunction, paravalvular leak, and tamponade. A double thoracotomy was performed for hemothorax and infection (1 side with pleurodesis). He was referred for heart transplantation because of persistent paravalvular leak, aortic failure, and constrictive pericarditis, with repeated hospital admissions for heart failure. At the time of hospitalization, the patient was in New York Heart Association functional class IV. In addition, he presented a pseudoaneurysm of the ascending aorta, at the level of the pulmonary artery. A 2-stage procedure was decided based on the following factors: an incompetent aortic valve, presence of an ascending aortic aneurysm, lack of a complete artificial heart, and foreseeable extremely complex cardiectomy with a high risk of graft loss due to lengthy ischemia time. The strategy consisted of a cardiectomy and establishment of biventricular assistance in the first stage, and transplantation in the second stage.
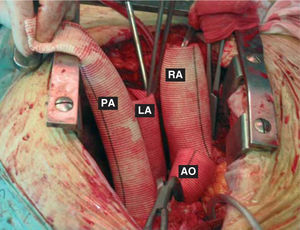
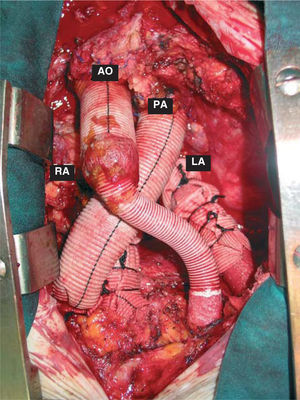
The images show the outcome of the cardiectomy, in which both ventricles were removed and the atrial remnants left in place. Figure 1 shows the grafts after anastomosing to the right atrium (RA), left atrium (LA), pulmonary artery (PA), and aorta (AO). In Figure 2 the grafts are in the definitive position and connected to the Thoratec® left ventricular assist devices (LVADs).

Figure 1.

Figure 2.
At 34 days of ventricular assistance, an orthotopic heart transplantation was performed. Ultimately, the patient died due to primary graft failure.