To the Editor:
"Atypical" aortic coarctation (AAC) is a rare clinical entity that includes involvement of the ascending thoracic aorta, the descending thoracic aorta distal to the aortic isthmus, and the abdominal aorta. Abdominal aortic coarctation is present in 1% to 2% of all patients with aortic coarctation and is an unusual cause of essential hypertension in adults. AAC is caused by focal stenosis or a hypoplastic segment of the aorta, is most often found at the renal level, and is frequently related to stenosis of the renal arteries (60%) or mesenteric arteries (30%).1
AAC has several causes, both congenital and acquired, although the latter are more common. Among the potential causes of acquired origin, the most common is Takayasu arteritis.2
The typical clinical presentation in young patients is hypertension in the upper limbs and a decrease or lack of pulses in the legs.1 In addition to the clinical history, the diagnosis is supported by noninvasive imaging tests, such as contrast-enhanced computed tomography (CT angiography), magnetic resonance imaging, and transesophageal echocardiography.3 Catheterization, the definitive diagnostic method, demonstrates the arterial pressure gradient across the stenosis.
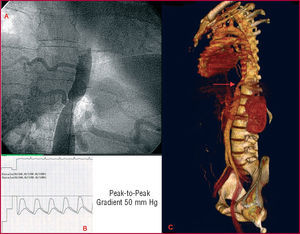
We describe a 28-year-old man who underwent study for essential hypertension. The examination showed normal physical development, blood pressure in the arms of 165/97 mm Hg, decreased pulses in the legs, and a systolic bruit, localized to the epigastrium. Transthoracic echocardiography revealed preserved ventricular function with mild left ventricular hypertrophy, but no other valvular or descending thoracic aorta abnormalities. CT angiography, performed to assess the abdominal aorta (Figure 1C), showed an abdominal aortic coarctation 2 cm in length distal to the diaphragmatic hiatus, and considerable collateral circulation that did not affect the celiac trunk or renal artery outflow. Cardiac catheterization revealed a peak-to-peak gradient of 50 mmHg in the hemodynamic study; the abdominal aortography showed a minimum lumen diameter of 9 mm, with reference diameters of 20 mm for the proximal abdominal aorta and of 24 mm for the distal (Figure 1A and B).

Figure 1. Initial diagnosis.
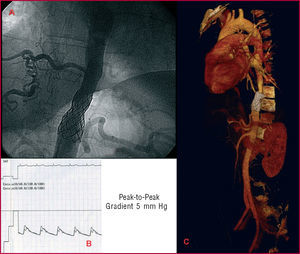
Based on the CT angiography and aortography findings, percutaneous treatment of the coarctation was performed. The procedure used a right femoral access with a 12F sheath, and expansions were performed with a 16-mm diameter PDZ649 balloon (Numed Inc., Hopkinton, USA) and a 20-mm Maxi LD balloon dilatation catheter (Cordis, Johnson & Johnson, USA) in the coarctation. A residual peak-to-peak gradient of 27 mm Hg remained. Therefore, a CP8Z45 stent (Numed Inc.) coupled with a 20-mm balloon-in-balloon catheter (Numed Inc.) was implanted, obtaining a final residual gradient of 5 mmHg (Figure 2A and B). Six months later, the patient was asymptomatic with normal blood pressure values and no need for antihypertensive therapy. CT angiography performed during follow-up confirmed proper positioning of the intravascular device (Figure 2C).

Figure 2. Postangioplasty results.
Aortic coarctation in adults has been traditionally treated by surgical aorto-aortic (end-to-end) bypass, although studies of patients with thoracic aortic coarctation treated with percutaneous angioplasty or stent placement have been published in the past 10 years.4,5 In the case of AAC, there are no studies comparing the long-term outcome in adult patients depending on the treatment used. Therefore, the best therapeutic option should be assessed by considering several aspects, such as the anatomy of the aorta (tortuous vessels, length of the hypoplastic segment), stenosis in other arteries (renal, mesenteric), and the trans-coarctation gradient.2 Surgery should be considered mainly in patients with abdominal aortic coarctation who present tortuous aortas and severe gradients or who have associated stenosis of the renal or mesenteric arteries. The long-term prognosis depends mainly on blood pressure control and the underlying disease; thus, Takayasu disease has a poorer prognosis.2
In conclusion, AAC is a rare cause of hypertension in adult patients and percutaneous treatment may be an excellent alternative in selected cases. There are no published series describing case studies of adult patients with AAC treated percutaneously with stent placement; hence, the long-term progress of these cases is unknown.