
Dear Editor,
Blunt chest trauma is most commonly seen after motor vehicle accidents, but also occurs during sporting activity. The prevalence of cardiac complications after such trauma varies between 2.6% and 4.5%.1 These complications are mainly the result of myocardial contusion, which can be associated with complications similar to those of myocardial infarction.2
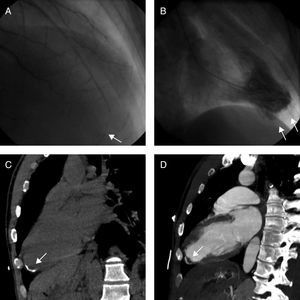
Here we describe the case of a 44–year-old male full-contact fighter who experienced sudden onset of palpitations associated with oppressive chest pain during sexual intercourse. He confessed that he had been taking oral anabolic-androgenic steroids for one month. Pre-hospital electrocardiogram showed a ventricular tachycardia (VT) originating from the left apical wall (Figure 1). After intravenous bolus of amiodarone, VT converted to atrial fibrillation and subsequently to sinus rhythm. Coronary angiogram showed a 30% narrowing in the mid-segment of a non-dominant right coronary artery. The left coronary arteries were angiographically normal except for a distal left anterior descending coronary artery of very small diameter (Figure 2A). Left ventriculogram revealed a preserved ventricular function with a calcified apical aneurysm (Figure 2B). Thoracic computed tomography without contrast confirmed that the apical aneurysm was calcified; post-contrast exam showed a small mural thrombus (Figure 2C and D).

Figure 1. Extra-hospital electrocardiogram showing ventricular tachycardia originating from the left apical wall.

Figure 2. Coronary angiogram (right anterior oblique 10 cranial 40 projection) showing a very small diameter distal left anterior descending coronary artery (A). Left ventriculogram (right anterior oblique projection) showing a preserved ventricular function with a calcified apical aneurysm (B). Thoracic computed tomography without contrast confirmed that the apical aneurysm was calcified (C). Post-contrast exam showing a small mural thrombus (D).
In blunt chest trauma, direct damage to the coronary arteries is not common. Because of its anterior location, left anterior descending coronary artery is the most frequenty affected vessel, followed by the right coronary artery. Cases of sports-related traumatic coronary dissection have been reported following waterskiing and cycling accidents, and after collision between players during basketball, soccer, and rugby games.3
In the case of repeated chest trauma from boxing, pericardial constriction caused by chronic hemopericardium has been described.4 We now report a calcified apical aneurysm with apical left anterior descending coronary artery abnormality as a probable consequence of asymptomatic cardiac contusion in a patient who had competed in full-contact fighting for many years, and had been knocked out by a strong hit to the chest several years previously. He presented years later with a VT derived from that scarring, probably triggered by anabolic-androgenic steroid use.5 Possible mechanisms to explain this coronary damage principally include epicardial hematoma with external compression; coronary artery dissection, vessel rupture or plaque rupture with thrombosis are possible alternatives. Apart from his fighting activity, no other established factor for apical aneurysm was found.
Internal cardioverter defibrillator implantation was indicated in secondary prevention, and the patient agreed to stop fighting. At the one-year follow-up, despite administration of betablockers, internal cardioverter defibrillator interrogation revealed numerous non-sustained VTs, but no shock was delivered.
The unusual feature of this case is the presence of structural cardiac injury following blunt chest trauma. To our knowledge, calcified apical aneurysm has never been described in association with combat sports.
Corresponding author: stephane.noble@hcuge.ch