To the Editor:
Idiopathic left ventricle tachycardia (ILVT) is an uncommon form of ventricular tachycardia (VT) that is seen in young patients without structural heart disease. Whereas medical treatment is only palliative, radiofrequency (RF) catheter ablation is curative in majority of patients.1 However, conventional RF ablation for ILVT has several inherent limitations. Procedure duration can be rather long and radiation exposure is therefore high. Moreover, septal location of the re-entrant circuit in this tachycardia makes the catheter manipulation difficult. The recently developed magnetic navigation system (MNS) facilitates more precise control of ablation catheters in the treatment of complex arrhythmias.2 Recent data support the hypothesis that these systems may offer advantages to classic catheter ablation procedures.3-5 The aim of this case report is to demonstrate the feasibility and potential benefits of using a stereotactic MNS for mapping and ablation of ILVT.
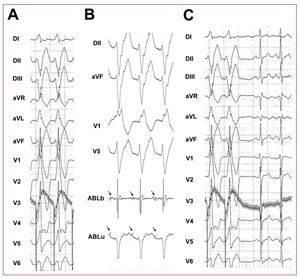
An 18-year-old man with a wide-QRS tachycardia without structural heart disease was referred for catheter ablation. Despite medical treatment, he had several recurrences, presenting unspecific symptoms of fatigue. The tachycardia had a rate of 160 beats/min and showed a right bundle branch block pattern with superior axis. An electrophysiology study was undertaken. Standard quadripolar electrophysiology catheter was inserted in the right ventricle. Sustained VT could be easily and reproducibly induced by rapid pacing (220 msec of cycle length) (Figure 1A). Through the femoral artery a magnetic navigation quadripolar catheter (Navistar-RMT 4 mm, Biosense-Webster, Inc, Diamond Bar, CA, USA) was introduced and advanced through the aortic valve to the left ventricle (LV) using a automatic catheter advancer system (CardiodriveTM, Stereotaxis, Stereotaxis Inc, St Louis, MO, USA) placed in the patient's thigh. The catheter was manoeuvred using the MNS (Niobe Stereotaxis MNS, Stereotaxis Inc.). The Niobe system consists of 2 large magnets, situated on either side of the patient and controlled via a computer workstation (Navigant, Stereotaxis Inc.) to allow for changes in the orientation of a stable magnet field within the chest of the patient. The ablation catheter has 3 magnets in the distal shaft that align themselves with the field produced by the external magnets, allowing for effective catheter orientation. Remote catheter advancement and retraction is performed with the catheter advancer system. After the magnets were brought in next to the perform patient, remote control of all of the components of the system was performed by the physicians from the control room.

Figure 1. Electocardiograms: A: 12 lead ECG showing typical morphology of idiopathic left ventricular tachycardia. B: ablation signals (bipolar and unipolar) demonstrationg stable Purkinje potentials (arrows). C: termination of tachycardia by RF ablation. ABLb indicates bipolar ablation signal; ABLu, unipolar ablation signal.
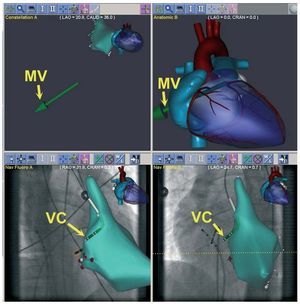
During tachycardia, an anatomical map of the LV was performed (CARTO-RMT, Biosense Webster, Tirat Hacarmel, Israel) (Figure 2). The ablation catheter was advanced to the LV apex. Using the MNS the septally oriented catheter was automatically pulled back using 3 mm steps. At each site Purkinje potentials (PP) were registered, and the vectors necessary to target all positions were stored in the Navigant system. At the end of the pull-back, the ablation catheter was easily redirected to the position where the earliest PP were recorded (Figure 1B) using the vectors previously stored in the workstation. Pace mapping at this site reproduced a 12/12 QRS morphology of the clinical tachycardia. RF energy delivery was performed during ongoing tachycardia, and ablation at this site terminated the tachycardia (Figure 1C). A total number of 6 applications were given in the area of interest, and no further tachycardia was inducible. Disappearance of PP in sinus rhythm was also demonstrated. The fluoroscopy time was 4.6 min and the procedure time was 150 min.

Figure 2. Navigant screen with the activation map integrated with the radiographic images (RAO, lower left pannel; LAO, lower right pannel); the system draws a virtual catheter according to the magnet vectors applied by the MNS (upper pannels). MV indicates magnet vector; VC, virtual catheter.
ILVT with right bundle branch block configuration and left-axis deviation is a rare form of VT that has been suggested to originate from the left-posterior fascicle. RF is a curative procedure for these patients. Successful ablation can be performed by targeting the earliest high-frequency Purkinje potential both during sinus rhythm and during tachycardia.6 However, this is not always possible, as conventional catheters cannot always be easily directed to the site of interest when using a retrograde approach, resulting in prolonged x-ray exposures and procedure times.
Using floppy catheters guided by MNS permit more accurate catheter manipulation during technically challenging ablation procedures, or in patients with complex heart anatomy. Complications such as mechanically induced arrhythmias are less prone to appear. Moreover, virtual, real-time catheter location allows less use of fluoroscopy in catheter positioning and manipulation. Apart from the advantages to the physician (reduction in radiation-exposition time and less postural stress), these tools may help to reduce the usually prolonged duration and fluoroscopy times of conventional manual procedures. The clear advantage of catheter stability is an asset for electrophysiology interventions.
This case clearly demonstrates that using MNS to treat ILVT is feasible and effective, and it may help to overcome some of the disadvantages of classic approach to this arrhythmia. In the future, these and other innovative advances in technology may facilitate the current practice of catheter ablation of ILVT and other even more complex arrhythmias.