To the Editor:
A 38-year-old man with hypertrophic cardiomyopathy was referred to the hospital for an electrophysiological study of paroxysmal tachycardias. The electrocardiogram (ECG) was normal. Four multipolar catheters were introduced into the right atrium (RA), the His bundle, right ventricular (RV) apex, and the coronary sinus (CS). A narrow QRS complex orthodromic tachycardia with a cycle length of 320 ms was induced from RA through a left anterolateral Kent bundle (Figures 1A and 2A). An extrastimulus test delivered from CS revealed a progressive prolongation of the AH and AV intervals, with simultaneous shortening of the HV interval and a QRS morphology indicative of right bundle branch block and anterior hemiblock. These findings were compatible with a Mahaim accessory pathway connected to posteroseptal left ventricle or left posterior fascicle. A second, slower reentry tachycardia was induced from CS, with retrograde conduction through left Kent bundle, and preexcited through the Mahaim pathway (Figure 2B). During the study, different widths and frequencies of the preexcited tachycardia were observed (Figures 1B and 1C). Entrainment of these tachycardias from RV (Figures 1B and 1C) resulted in an advance in left atrium and fusion of the next QRS complex, revealing the anterograde depolarization of the His bundle (in the proximal to distal direction with an HV interval of 10 ms) (Figure 2B). No retrograde His bundle tachycardia was observed in the QRS complex. The late atrial extrastimuli in CS either occurred in the refractory period or interrupted the tachycardia due to the early invasion of left atrium by the left-sided pathway. The Kent bundle was interrupted by radiofrequency. Subsequently, there was no ventriculoatrial conduction, nor was it possible to induce preexcited tachycardia. A slow Mahaim bundle potential was observed in the posterolateral mitral annulus; at this point, the application of radiofrequency, with the appearance of automatic rhythm, interrupted the accessory pathway (Figure 2C).

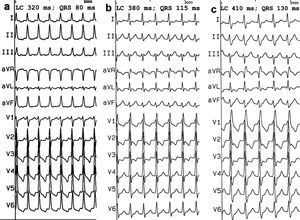
Figure 1. Electrocardiogram of the orthodromic tachycardia without preexcitation (A); more preexcited by the Mahaim than by the atrioventricular node (C); intermediate between the two (B). LC indicates cycle length.

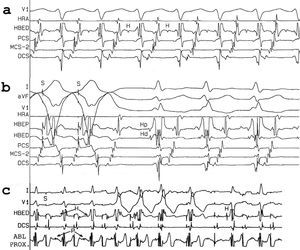
Figure 2. A: orthodromic tachycardia due to left-sided Kent (HV 45 ms). B: entrainment of the tachycardia. C: ablation of the Mahaim. ABL-PROX indicates proximal ablation; HBEP/HBED, proximal and distal His; HRA, right atrium; P, potential; PCS, MCS-2, DCS, proximal, mid- and distal coronary sinuses; S, stimulus.
The so-called "Mahaim fibers" are connections between RA and the right branch (atriofascicular) or RV (atrioventricular [AV]), and are rarely nodofascicular or nodoventricular. Physiologically, they have long conduction times and node-like decremental properties, and retrograde conduction is absent.1,2 They are located in the posterolateral tricuspid annulus, communicated in a few cases in which the morphology of the preexcited ECG indicates a left ventricular insertion.3-6 In these patients, the electrophysiological descriptions of the atrial insertion or nodal and ventricular insertion are incomplete or are unclear. Some of them did not have associated tachycardias and ablation was not performed. The case has been reported of a patient with a left Mahaim fiber in whom ablation guided by the pathway potentials was performed.4
Our case is peculiar because of the association between a left posterolateral Mahaim fiber and an occult left anterolateral Kent bundle. In our opinion, the decremental pathway has an innocent bystander behavior in the orthodromic tachycardia. When the AV node conduction is rapid, probably due to autonomic changes, the ventricular preexcitation is not exteriorized as the impulse travels exclusively through the AV node. When the nodal conduction is slower, the QRS complex results from the fusion of the impulse through the decremental accessory pathway, with long, constant conduction times (left ventricular or left posterior fascicular activation) and the AV node (right bundle branch activation). Different degrees of delay in the AV node would result in different degrees of fusion and would change the morphology of the preexcited tachycardias (the lower the frequency, the greater the preexcitation) (Figure 1). During preexcited tachycardia, the His bundle is anterograde and activated via the AV node (proximal His prior to distal His). Thus, one or more fusion beats may be observed during tachycardia. This fusion would not occur if the His bundle had been activated retrogradely from the Mahaim. The bystander condition is confirmed as no further tachycardia was induced following the interruption of the Kent pathway. The left atrial insertion of the Mahaim is unequivocal as a slow potential, characteristic of the mitral annulus, was recorded.