To the Editor:
Bilateral common carotid artery occlusion (CCAO) is a rare vascular disease. In CCAO collateral circulation feeding the carotid arteries usually comes from the vertebrobasilar system. We report a bilateral CCAO with uncommon collateral circulation arising from both vertebral-basilar and dilated superior thyroid arteries, further submitted to successful surgical myocardial revascularization under extracorporeal circulation.
A 53-year-old-man was admitted to our institution complaining of dizziness, daily episodes of bilateral amaurosis fugax, lasting up to 1 minute, for the past 18 months. He also described daily episodes of class III typical angina (CCS) and class III dyspnea (NYHA). He denied any other symptoms. He had a past history of systemic arterial hypertension and dislipidemia, and positive familial history for coronary artery disease before 60 years old, in 2 first degree relatives. He had no history of diabetes mellitus and denied any previous tobacco use. On physical examination, the carotid pulses were bilaterally absent, but a pansystolic murmur was heard in both sides of the neck. Cardiac auscultation revealed a fourth heart sound. Neurological and ophthalmologic examinations were normal. Heart rate was 56 bpm, right upper limb blood pressure was 180/90 mm Hg, and 170/90 mm Hg on the left upper limb. His BMI was 23.2 kg/m2.
Left ventricular systolic function was preserved in 2-D echocardiogram. Carotid duplex scanning showed bilateral CCAO at their origin, and patent internal and external carotid arteries in addition to unusual reversed flow from superior thyroid arteries into carotid arteries were observed bilaterally (Figure, A and B). High-resolution MRI angiography confirmed bilateral CCAO exclusion and bilateral abnormally dilated superior thyroid arteries (Figure, C and D). Aortic arch angiogram demonstrated CCAO at their origin and protected vertebral arteries supplying the circle of Willis (Figure, E and F). Attending physicians concurred in that cerebral circulation was functionally preserved by compensatory circulation. Additional coronary angiography revealed severe obstruction affecting both left main ostium and right coronary artery.

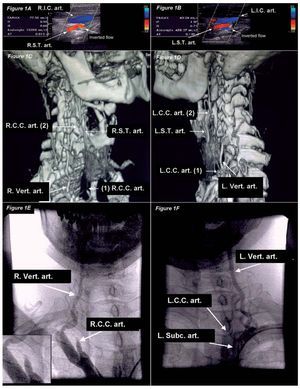
Figure 1. A and B: color Doppler ultrasound of cervical vessels showing right (A) and left (B) superior thyroid arteries supplying carotid arteries bilaterally (note inverted red-colored flow in superior thyroid arteries). C and D: magnetic resonance virtual angiography imaging shows exclusion of both right (C) and left (D) common carotid arteries. Note inferior—mark (1)—and superior—mark (2)—cut-off edges of common carotid arteries bilaterally. Remarkable compensatory dilation of both superior thyroid arteries supplying respective carotid arteries above occlusion level superiorly—mark (2)—is noted; in C, note that superior thyroid artery converges to common carotid artery above occlusion level—mark (2)—. Note on the rightside panel (C) that occlusion level occurs proximally to carotid artery bifurcation— mark (2)—, whereas on the left-side panel (D), occlusion is observed at carotid bifurcation level. E and F: right (E) and left (F) cervical angiography shows common carotid artery exclusion; note the stop edge of right common carotid artery at its emergence from brachiocephalic trunk (inset on the left). LCC art indicates left common carotid artery; LIC art, left internal carotid artery; LST art, left superior thyroid artery; L subc art, left subclavian artery; l vert art, left vertebral artery; R Vert art, right vertebral artery; RCC art, right common carotid artery; RIC art, right internal carotid artery; RST art, right superior thyroid artery.
After a thorough multidisciplinary round, it was concluded that surgical intervention on coronary lesions should be preferred exceptionally in present case, considering, first, the functionally preserved cerebral circulation; second, current high risk for coronary events in the short-term. Coronary artery bypass graft surgery was successfully carried out with left internal thoracic artery to the left anterior descending coronary artery and a saphenous vein graft to the right coronary artery. Surgical strategy was decided according to surgical team expertise aiming at reducing on-pump time. Extracorporeal circulation time was 90 minutes and the aortic cross-clamping time was 66 minutes. On the 60th postoperative day he was free of chest pain and remained neurologically stable.
Bilateral CCAO is a rare vascular disease often associated with sustained neurological deficits and poor prognosis.1 Unlike our patient, stroke has been the most common clinical presentation,2 and asymptomatic cases have been reported more frequently in unilateral CCAO. To the best of our knowledge, this is the first report of bilateral CCAO with unusual circulatory compensation of both internal and external carotid arteries arising from ipsilateral superior thyroid arteries, presenting mild neurological symptoms. No information has been found in the literature regarding an optimal revascularization approach similar to the present case.