Since 1993, successive health plans launched by the Department of Health in Catalonia (7.6 million inhabitants) have prioritized the management of cardiovascular diseases.1 Although mortality from these diseases has declined worldwide, including in Catalonia, they still caused 24.8% of deaths in 2018 (23.5% in men and 27.7% in women),2 representing the second cause of mortality in the study context. In 2019, there were 120 000 hospital admissions for cardiovascular diseases (11.3% of all admissions), of which 10 154 were for acute myocardial infarction.3
Catalonia's Strategic Framework for Cardiovascular Diseases4 (Pla Director en l’àmbit de les Malalties Cardiovasculars [PDMCV]), launched in 2006, prioritized the management of acute myocardial infarction with ST-segment elevation (STEMI). At that time, the annual rate of percutaneous coronary interventions (PCI) in Catalonia was 978 per million inhabitants,5 the lowest in Spain (1161 per million inhabitants). The rate of primary PCI per million inhabitants was 104 in Catalonia but was 187 in Spain. Moreover, the scarce data available showed that about a third of STEMI did not receive any reperfusion procedure.6 Therefore, the PDMCV launched the Acute Myocardial Infarction Code (AMI Code) to increase the number of PCI in STEMI and to reduce the time between electrocardiogram (ECG) performance and PCI to less than 120minutes.
Briefly, the AMI Code is an emergency protocol that includes 3 key issues. First, urgent identification of STEMI by an ECG performed at the first point of care. Second, the activation of the Code if there is STEMI, left-branch blockade, or acute coronary syndrome suspicion. Third, the division of Catalonia (32 000 km2; 7.6 million inhabitants) in 10 areas with a referral hospital in each one.7,8 These centers are legally required to accept the emergency and prioritize direct access to the cath lab.
The AMI Code began on June 1, 2009, with the agreement between the Department of Health, the Catalan Health Service, the Catalan Medical Emergencies System, the professional associations representing the parties involved (Cardiology, Emergencies, Intensive Care, Primary Care), and the managers of the assigned referral hospitals. The legal framework for the AMI Code laid down the need for a specific registry (Codi IAM registry) as a key tool for the implementation and management of the AMI Code, the surveillance of the epidemiological and clinical data, and the evaluation of the trends of the activity and results in our country.
Goals of the registryThe Codi IAM registry is a prospective database of AMI Code episodes that integrates clinical information and management variables about the process with the aim of improving a unique standard of care for the 7.6 million inhabitants of Catalonia. Time variables, such as door-to-balloon time, are crucial. Other specific goals are to gather high-quality data on the epidemiological and clinical characteristics of STEMI patients, to evaluate the impact of the AMI Code on mortality, and to enhance quality improvement through benchmarking of the performance of the centers. Finally, the real-world data gathered in the registry enables research on clinical and management issues.
Data securityThe Codi IAM registry is overseen by the legal framework of public mandatory health care registries and was developed within a secure platform integrated into the Systems Plan of the Catalan Health Service. All the data are anonymized. Each hospital is responsible for recording their own cases on the platform through secure login passwords, and they only have access to data deemed necessary for their clinical and/or administrative positions.
Governance and organizationThe governance of the AMI Code relies on a monitoring committee composed of a representative of each of the 10 hospitals, professional scientific associations, and the health care authorities (PDMCV and Catalan Health Service). The main function of this committee, which meets periodically, is to supervise the functioning of the AMI Code.
A technical office, under the aegis of the Catalan Health Service, is in charge of the daily management of the registry and updating of the publicly available manual.9 In addition, a technical committee reviews and updates the variables included in the registry according to the European cardiology guidelines.10
There is also a scientific committee, composed of professionals from different participating centers, to promote research within the scope of the program, and to guarantee the proper use of registry data and the quality of publications. The scientific committee issues an annual competitive call for research proposals. To date, more than 10 proposals have been funded, and numerous scientific communications, 20 publications and 4 doctoral theses have been produced.
Registry frameworkThe inclusion criteria of the AMI Code considers all the STEMI cases attended in the first 12hours of chest pain onset. Exclusion criteria are applied in those cases with nondiagnostic ECG, more than 12hours of pain and less than 12 months of life expectancy. Since 2013, the Catalan Medical Emergencies System has registered, through the web service, all the cases attended. These cases are merged with those registered from referral hospitals through a unique identification number for each episode and patient.
The content of the Codi IAM registry has evolved from time variables almost exclusively, needed for the management of the AMI Code, to the inclusion of an increased number of clinical variables. Currently, the variables gather information on patient identification and demographic characteristics, the first assistance, time variables such as onset of pain, call, initial contact, ECG, diagnosis, therapeutic decision, the start of the transfer, door-balloon time, clinical conditions, therapeutic procedures, drug administration—including antiplatelet and anticoagulant treatment—medical complications, in-hospital mortality, and final diagnosis. Data provided by the Catalan Medical Emergencies System include variables of geolocation in the first assistance and therefore allow mapping the activated codes and identification of delay times.
Moreover, the Codi IAM registry collects data on mortality in the first 24hours, at 30 days, and at 12 months. Furthermore, data from the registry can be linked, through the unique identification number of each citizen, with other public health care databases in the same manner with discharges, drugs prescription, emergencies, and primary health care.
One of the keys to the success of the AMI Code is the coresponsibility of different professionals in the whole process (appendix 1). Each professional receives specific training and participates in frequent meetings with the technical office to improve the quality of the data. In addition, some automatic filters, such as time filters or quality control indicators, have been implemented to avoid mistakes, incongruences, or duplications to the registry.
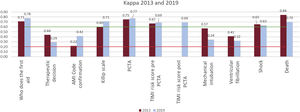
There have been 2 audits (2013 and 2019) to explore the agreement between data from the registry and those of the medical records of the hospitals. The audits examined the data forms of 340 and 419 patients recruited in 2013 and 2019, respectively. These cases were selected through proportional stratified random sampling by center. In both audits, the kappa values were higher than 0.6 in the key variables of the AMI Code, showing a very good match in the time variables (figure 1). In addition, the match between the cases reported by the Catalan Medical Emergencies System and those registered in the hospital was 98%. The agreement in the episodes between the registry and the hospitals’ discharge data set was greater than 85%, reaching 90% in the case of STEMI episodes.

Kappa values of main variables in clinical registries and the Codi IAM registry from the 2013 and 2019 audits. Kappa values: > 0.80, very good agreement; 0.61-0.80, good agreement; 0.41-0.60, moderate agreement; 0.21-0.40, fair agreement; < 0.20, poor agreement. AMI, acute myocardial infarction; PCTA, percutaneous coronary transluminal angioplasty; TIMI, Thrombolysis in Myocardial Infarction.
All this reliable information is useful to optimize AMI Code management. A specific health care registry completed by all the public network centers is probably the most useful information source, as it also allows monitoring of clinical and operational issues of the health care process from the onset of pain until 30 days after discharge. The robustness of the data and their usefulness for the management of the AMI Code compensate for the enormous efforts made to constantly complete the registry. The analysis of the information indicates that the AMI Code has improved the health care process, achieving an organizational transformation and better coordinated patient flow.
From 2010 to 2020, 39676 AMI patients were included in the registry, of whom more than 80% were appropriate. The median time between the performance of the ECG and PCI decreased from 122minutes to 94, and the percentage of patients with PCI performed less than 120minutes after the ECG increased from 58% to 71%. In the last 25 years, the rate of STEMI per million inhabitants has also increased, from 387.5 to 541.5 and the rate of PCI has increased from 76 to 381.1 per million inhabitants. Mapping of the data has helped to identify which territories needed improvement. This analysis has been useful to justify the extension of the schedule of the cath labs and has allowed decision-making on the inadvisability of remote ECG transmission.
Population-based registries have some limitations, especially from the point of view of clinical information, which is usually partial. However, they can provide useful information on the performance in the real world of the introduction of novel therapeutic strategies and to estimate their effectiveness, in what has been called real-world evidence. The organization of the scientific committee has stimulated research taking advantage of a prospective, long-term database that includes real-world data.
The AMI Code has led to a paradigm shift in Catalan health care for several reasons. Apart from the fact that the Code can be activated by the Catalan Medical Emergencies System, which saves time, it includes not only in-hospital care but also prehospital care. Involvement in the Registry of the Catalan Ministry of Health, which regulates all the decisions concerning patients’ health care pathway, resulted in a strong commitment from all public hospitals involved and facilitated the best use of cath labs. In addition, the success of the code has been an incentive for improving the management of other emergencies. Finally, the registry led to a change in the relationship between health care administration and clinicians toward greater collaboration. The Codi IAM registry, an exhaustive, reliable and useful tool to assess the management of the AMI Code, is one of the key factors that has improved patient care over the last 10 years and it will continue to do so in the coming years.
FUNDINGNone received.
CONFLICTS OF INTERESTM.T. Faixedas and M.J. Pueyo declare no conflicts of interest. J. Mauri declares honoraria from Abbott, Medtronic and Biosensors for lectures and educational events.
The authors wish to express their gratitude to the registrars Helena Tizón Marcos, Manel Piqué, Carlos Tomás-Querol, Mónica Masotti, Ander Regueiro, Rut Andrea, Oriol de Diego, Xavier Carrillo, Mercè Camprubí, Juan Francisco Muñoz, that have participated in the Codi IAM registry, and also to all the professionals who throughout these years have dedicated time and effort to maintain the quality of the registry.
María Teresa Faixedas, Josep Jiménez, Carmen Medina, Francesc Güell y Ariadna Sanz (Pla director de malalties cardiovasculars. Servei Català de la Salut, Barcelona, Spain). Ricard Tresserras (Direcció General de Planificació. Department de Salut, Generalitat de Catalunya, Spain). Josepa Mauri (Pla director de malalties cardiovasculars. Departament de Salut, Generalitat de Catalunya, Spain). Assumpta Ricart (Gerència de Processos Integrats, Servei Català de la Salut, Barcelona, Spain). María J. Pueyo (Unitat Transversal, Consorci Sanitari de Barcelona, Barcelona, Spain).