Tako-tsubo syndrome is a potentially serious disease during the acute phase. It mimics myocardial infarction, but with no potentially causative coronary lesions. The aim of this study was to analyze the clinical course and outcome of patients with tako-tsubo syndrome by sex.
MethodsWe analyzed the characteristics of patients included in the RETAKO registry from 2003 to 2015, a multicenter registry with participation of 32 Spanish hospitals.
ResultsOf 562 patients included, 493 (87.7%) were women. Chest pain was less frequent as an initial symptom in men than in women (43 [66.2%] vs 390 [82.8%]; P < .01). The prognosis was worse in men, with higher in-hospital mortality (3 [4.4%] vs 1 [0.2%]; P < .01), longer intensive care stay (4.2 ± 3.7 vs 3.2 ± 3.2 days; P = .03) and a higher frequency of severe heart failure (22 [33.3%] vs 95 [20.3%]; P = .02). However, dynamic obstruction at the left-ventricular outflow tract occurred exclusively in women (39 [7.9%] vs 0 [0.0%]; P = .02). The incidence of functional mitral regurgitation was also higher in women (52 [10.6%] vs 2 [2.9%]; P = .04).
ConclusionsTako-tsubo syndrome shows wide differences by sex in terms of its incidence, presentation, and outcomes. Prognosis is worse in men.
Keywords
Tako-tsubo syndrome (TTS) is a generally reversible episode of acute left ventricular systolic dysfunction of variable severity. First described in 1990 in Japan, TTS has a similar clinical presentation to acute myocardial infarction, but occurs in the absence of coronary lesions that could account for the myocardial injury in affected individuals; moreover, the clinical symptoms of TTS resolve rapidly, with ventricular contraction normalizing in a matter of days or weeks.1
The underlying mechanisms and pathophysiology of TTS are poorly understood; however, a mechanism has been proposed involving catecholamine-induced acute myocardial injury.2 One characteristic noted since the first TTS studies is a marked difference in incidence between the sexes, with the condition being much more common in women, especially after the menopause.3 Most published studies have reported a female-to-male patient ratio of around 9:1.4–6
Tako-tsubo syndrome was historically considered a benign condition; however, over the years many complications have been reported in the acute phase of the syndrome,7–11 especially in patients who develop heart failure.12 Likewise, follow-up has revealed recurrent episodes in some patients.13 More recent studies have revealed morbidity and mortality rates similar to or higher than those observed in patients with acute coronary syndrome.6
The early view of TTS as a benign disorder has therefore been replaced by recognition that the patient's clinical course can be affected by potentially serious complications, especially those appearing in the first hours or days. Given the marked differences in TTS incidence by sex, we analyzed whether the type of complications and prognosis also differ between men and women. Knowledge of any such differences could facilitate their detection and help to improve patient prognosis.
METHODSPatient InclusionThe data analyzed here are from the Spanish tako-tsubo registry (REgistro español de síndrome de TAKO-tsubo; RETAKO).5 RETAKO is a prospective study coordinated by the Ischemic Heart Disease and Acute Cardiovascular Care Section of the Spanish Society of Cardiology. Patient inclusion is voluntary. Diagnosis was confirmed by modified Mayo Clinic criteria.14
In this study, we analyzed data from TTS patients admitted consecutively to any of the 32 hospitals participating in RETAKO between January 2003 and December 2015. Records were compiled of clinical characteristics, in-hospital complications, analytical results, electrocardiograms, and the results of imaging analysis by echocardiograpy and other modalities available at each center (magnetic resonance imaging was optional in the protocal). Initially, this information was recorded on a case report form and sent by e-mail to a data processing center; from 2014, information was directly recorded in an online case report form. Inclusion was conditional on the patient having undergone an invasive coronary angiography investigation that excluded significant obstructive lesions (> 50%) and any other potential cause of the clinical symptoms (eg, thrombus, dissection, or ulcer). Treatment and follow-up were always at the discretion of the attending physicians. Except for those patients who died before follow-up, inclusion in the analysis required at least 1 follow-up imaging examination by any modality (usually echocardiography) showing complete normalization of the segmental contraction abnormalities diagnosed in the acute phase.
The study was approved by the Ethics Committee of Hospital Clínico San Carlos, and patients gave informed consent to participate in the registry.
Triggering FactorsWe recently proposed a classification of TTS according to its potential triggering factors.15 This classification distinguishes between primary forms, with no identifiable trigger or triggered by major psychological stress, and secondary forms, triggered by physical factors such as an asthma attack, surgery, trauma, or pheochromocytoma.16 The main interest of this classification is its prognostic implications; secondary TTS is associated with a worse short- and long-term prognosis.15 For the present analysis, possible triggering factors were noted during data collection, and patients were subsequently assigned to either the primary or the secondary TTS group.
ComplicationsWe analyzed the appearance of the following complications during hospitalization:
- •
Severe heart failure, defined as acute pulmonary edema or cardiogenic shock. The incidence of shock was also analyzed independently.
- •
Moderate or severe acute functional mitral regurgitation, with no recorded clinical history or with recovery during follow-up.
- •
Dynamic left ventricular outflow tract (LVOT) obstruction. Obstructions were determined echocardiographically or from catheter pressure recordings, and obstructions > 25mmHg were were considered significant.3
- •
Major bleeding (anemia with a hemoglobin drop ≥ 2g/dL or requiring transfusion).
- •
Others: intraventricular thrombus formation, systemic embolism and stroke, pulmonary thromboembolism, pericarditis, recurrent TTS during hospitalization, acute renal failure, in-hospital infection, catheterization complications, and in-hospital death.
Data were analyzed with STATA, version 12.1 (StataCorp, United States). The study is descriptive. Continuous variables are expressed as mean ± standard deviation, and differences were analyzed by the Student t test or the Wilcoxon rank sum test for nonnormal distribution. Categorical variables are expressed as frequency and percentage and were compared by the chi-square test or by the Fisher exact test for nonnormal distribution. Differences were considered significant at P <.05.
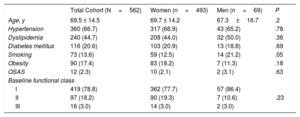
RESULTSStudy PopulationA total of 562 patients were included. The mean age was 69.5 ± 14.5 years, and 493 (87.7%) of the patients were women. No significant between-sex differences were observed for age, cardiovascular risk factors, or baseline functional class. A higher smoking prevalence was noted among men (Table 1).
Baseline Patient Characteristics for the Total Cohort and Grouped by Sex
| Total Cohort (N=562) | Women (n=493) | Men (n=69) | P | |
|---|---|---|---|---|
| Age, y | 69.5 ± 14.5 | 69.7 ± 14.2 | 67.3±16.7 | .2 |
| Hypertension | 360 (66.7) | 317 (66.9) | 43 (65.2) | .78 |
| Dyslipidemia | 240 (44.7) | 208 (44.0) | 32 (50.0) | .36 |
| Diabetes mellitus | 116 (20.6) | 103 (20.9) | 13 (18.8) | .69 |
| Smoking | 73 (13.6) | 59 (12.5) | 14 (21.2) | .05 |
| Obesity | 90 (17.4) | 83 (18.2) | 7 (11.3) | .18 |
| OSAS | 12 (2.3) | 10 (2.1) | 2 (3.1) | .63 |
| Baseline functional class | ||||
| I | 419 (78.8) | 362 (77.7) | 57 (86.4) | .23 |
| II | 97 (18.2) | 90 (19.3) | 7 (10.6) | |
| III | 16 (3.0) | 14 (3.0) | 2 (3.0) | |
OSAS, obstructive sleep apnea syndrome.
Data are expressed as No. (%) or mean±standard deviation.
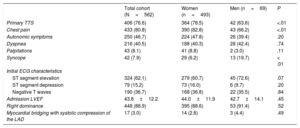
A significantly higher proportion of women than men were classified as having primary TTS: 364 (78.5%) vs 42 (63.6%); P <.01.
Clinical PresentationThe most frequent symptom on presentation was chest pain; however, this symptom was significantly less frequent in men than in women (43 [66.2%] vs 390 [82.8%]; P <.01). In contrast, syncope was more frequent among men than women (13 [19.7%] vs 29 [6.2%]; P <.01). No major between-sex differences were observed for other symptoms recorded on admission: palpitations, shortness of breath, or autonomic symptoms (Table 2).
Clinical Presentation of Tako-tsubo Syndrome
| Total cohort (N=562) | Women (n=493) | Men (n=69) | P | |
|---|---|---|---|---|
| Primary TTS | 406 (76.6) | 364 (78.5) | 42 (63.6) | <.01 |
| Chest pain | 433 (80.8) | 390 (82.8) | 43 (66.2) | <.01 |
| Autonomic symptoms | 250 (46.7) | 224 (47.8) | 26 (39.4) | .20 |
| Dyspnea | 216 (40.5) | 188 (40.3) | 28 (42.4) | .74 |
| Palpitations | 43 (8.1) | 41 (8.8) | 2 (3.0) | .11 |
| Syncope | 42 (7.9) | 29 (6.2) | 13 (19.7) | < .01 |
| Initial ECG characteristics | ||||
| ST segment elevation | 324 (62.1) | 279 (60.7) | 45 (72.6) | .07 |
| ST segment depression | 79 (15.2) | 73 (16.0) | 6 (9.7) | .20 |
| Negative T waves | 190 (36.7) | 168 (36.8) | 22 (35.5) | .84 |
| Admission LVEF | 43.8±12.2 | 44.0±11.9 | 42.7±14.1 | .45 |
| Right dominance | 448 (88.9) | 395 (88.6) | 53 (91.4) | .52 |
| Myocardial bridging with systolic compression of the LAD | 17 (3.0) | 14 (2.8) | 3 (4.4) | .49 |
ECG, electrocardiogram; LAD, left anterior descending coronary artery; LVEF, left ventricular ejection fraction; TTS, tako-tsubo syndrome.
Data are expressed as No. (%) or mean±standard deviation.
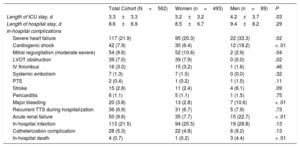
Men had a worse prognosis, with higher incidences of severe heart failure (33.3% vs 20.3%; P=.02), cardiogenic shock (18.2% vs 6.4%; P <.01), and in-hospital mortality (4.4% vs 0.2%; P <.01). Men also had a higher rate of major bleeding (10.6% vs 2.8%; P <.01), a higher incidence of acute renal failure (22.7% vs 7.7%; P <.01), and a longer mean stay in intensive care (4.2 days vs 3.7 days; P=.03).
In contrast, dynamic LVOT obststruction was observed only in women (7.9%), and the incidence of moderate-to-severe acute mitral regurgitation was also lower in men (2.9% vs 10.6%; P=.04).
There was no between-sex difference in left ventricular ejection fraction (42.7% ± 14.1% in men vs 44.0% ± 11.9% in women; P=.45) (Table 3).
Clinical Course and Complications
| Total Cohort (N=562) | Women (n=493) | Men (n=69) | P | |
|---|---|---|---|---|
| Length of ICU stay, d | 3.3±3.3 | 3.2±3.2 | 4.2±3.7 | .03 |
| Length of hospital stay, d | 8.6±6.9 | 8.5±6.7 | 9.4±8.2 | .29 |
| In-hospital complications | ||||
| Severe heart failure | 117 (21.9) | 95 (20.3) | 22 (33.3) | .02 |
| Cardiogenic shock | 42 (7.9) | 30 (6.4) | 12 (18.2) | < .01 |
| Mitral regurgitation (moderate-severe) | 54 (9.6) | 52 (10.6) | 2 (2.9) | .04 |
| LVOT obstruction | 39 (7.0) | 39 (7.9) | 0 (0.0) | .02 |
| IV thrombus | 16 (3.0) | 15 (3.2) | 1 (1.6) | .46 |
| Systemic embolism | 7 (1.3) | 7 (1.5) | 0 (0.0) | .32 |
| PTE | 2 (0.4) | 1 (0.2) | 1 (1.5) | .11 |
| Stroke | 15 (2.8) | 11 (2.4) | 4 (6.1) | .09 |
| Pericarditis | 6 (1.1) | 5 (1.1) | 1 (1.5) | .75 |
| Major bleeding | 20 (3.8) | 13 (2.8) | 7 (10.6) | < .01 |
| Recurrent TTS during hospitalization | 36 (6.9) | 31 (6.7) | 5 (7.9) | .73 |
| Acute renal failure | 50 (9.6) | 35 (7.7) | 15 (22.7) | < .01 |
| In-hospital infection | 113 (21.5) | 94 (20.5) | 19 (28.8) | .13 |
| Catheterization complication | 28 (5.3) | 22 (4.8) | 6 (9.2) | .13 |
| In-hospital death | 4 (0.7) | 1 (0.2) | 3 (4.4) | < .01 |
ICU, intensive care unit; IV, intraventricular; LVOT, left ventricular outflow tract; PTE, pulmonary thromboembolism.
Data are expressed as No. (%) or mean±standard deviation.
This study confirms the existence of substantial differences in the manifestation of TTS in men and women, including a 9-fold higher incidence in women. More importantly, our results also reveal significant between-sex differences in the clinical course of TTS during hospitalization. There were no overall between-sex differences in left ventricular ejection fraction, a widely used parameter for determining the severity of a TTS episode. Despite this, men had a worse in-hospital prognosis, with higher mortality, longer periods in intensive care, a higher risk of severe hemodynamic instability, and higher rates of major bleeding and renal function impairment. Nonetheless, LVOT obstruction and mitral regurgitation were more frequent among women. This information will be useful to physicians attending TTS patients by facilitating early detection of these complications.
Some of the results presented here have been reported in previous studies. The approximately 9-fold higher TTS incidence in women has been widely reported.4–6 The more frequent diagnosis based on chest pain in women and the higher frequency of severe hemodynamic instability (cardiogenic shock) in men match the findings of a German-Austrian multicenter study with similar characteristics to ours, albeit with fewer patients.4 However, our study also identifies major between-sex differences not described in previous reports, including dynamic LVOT obstruction and mitral regurgitation during the acute phase, parameters not evaluated in the German-Austrian cohort.
Primary TTS was more common among women, although more than half of male patients also fell into this category. The higher frequency of primary TTS in women may help to explain, at least in part, the observed between-sex differences in complications and prognosis. Secondary TTS is triggered by physical factors, such as asthma attack, recent surgery, injury, and serious infection.15 In this patient group, it is therefore important to consider not only the specific properties of TTS, but also the underlying disease that triggers the condition; these patients are often hemodynamically unstable and are more likely to develop complications. However, the notably different prognosis of men and women with TTS likely also includes contributions from sex-determined factors. It is well established that male heart failure patients with left ventricular systolic dysfunction have a worse prognosis than women with the same condition; moreover, this difference is independent of left ventricular ejection fraction17,18 and is more pronounced in patients with nonischemic dilated cardiomyopathy than in ischemic patients.19
One of the possible complications during the acute phase is dynamic LVOT obstruction, although this is normally reversible, correcting as left ventricular systolic function improves.20 To our knowledge, the clear between-sex differences in the appearance of this complication have not been reported in previous studies. Few published series have reported the incidence of dynamic LVOT obstruction in TTS patients, and even fewer have identified the sex of patients with this condition. In line with our registry, a systematic analysis in a series of just 32 patients (31 women and 1 man) identified LVOT obstruction in 8 patients, all of them women.21 In addition to being women, the patients with LVOT were more elderly than other TTS patients, and all of them had a septal bulge (sigmoid septum).21 However, demographic studies have revealed no differences by sex in the prevalence of sigmoid septum in the general population,22–24 and therefore sigmoid septum cannot explain the higher incidence of dynamic LVOT obstruction among female TTS patients. Analysis of other conditions has revealed an association between female sex and a higher incidence of LVOT obstruction among patients diagnosed with hypertrophic cardiomyopathy.25,26 In TTS, the underlying cause of the sex-association may be a different spatial distribution of catecholaminergic receptors in the left ventricle myocardium, with a steeper base-to-apex gradient in women. The resulting excessive release of catecholamines2 could produce the observed difference in the classic pattern between strictly basal hypercontractility and akinesia in the middistal segments, thereby favoring the more frequent dynamic LVOT obstruction seen in women.
Another complication that was more frequent in women was mitral regurgitation, classified as moderate or severe. Two characteristic underlying mechanisms of functional mitral regurgitation could account for its appearance during the acute phase of TTS7,27: a) the most common mechanism is apical displacement of the mitral leaflet coaptation point (tethering), produced by the dilatation and altered contraction of the medioventricular segments, and b) the second mechanism is systolic movement of the anterior mitral leaflet in patients with dynamic LVOT obstruction; this mechanism is less frequent but has been described in several reports and can sometimes coexist with tethering. Our finding that one of these causative mechanisms (LVOT obstruction) occurred only in women in our cohort could help to explain, at least in part, the higher frequency of acute functional mitral regurgitation in TTS among women.
LimitationsThe characteristics of the registry impose some limitations on the study. The voluntary nature of study participation may have introduced an inclusion bias, resulting in some types of patients not being represented in the cohort. Inclusion in the registry required a coronary angiography examination to confirm the absence of coronary lesions that could explain the symptoms. However, not all patients underwent this test, potentially resulting in the exclusion of patients with TTS. This will mostly have affected very elderly patients or those with a history of severe comorbidities; in these situations, a physician may prefer to avoid the use of an invasive technique and opt for a more conservative approach even when the initial suspected diagnosis is acute coronary syndrome. In other instances, angiography may not have been possible due to the severity of the initial symptoms; this would have been the case, for example, of a patient in whom TTS caused sudden death. The requirement of a coronary angiography investigation may therefore have led to underestimation of the severity and frequency of complications. Although the study recorded a higher frequency of functional mitral regurgitation in women, no systematic record was compiled of the underlying mechanism. Finally, angiographic and other data were analyzed by the investigators in each center, without the intervention of a central laboratory.
CONCLUSIONSTako-tsubo syndrome is a disease process showing pronounced differences between the sexes. Not only was TTS 9 times more common in women, its clinical course also showed a major divergence between men and women, with an overall worse prognosis in men, who showed worse hemodynamic deterioration and a higher rate of in-hospital mortality. Despite this trend, dynamic LVOT obstruction was observed only in female TTS patients, who also had a higher incidence of functional mitral regurgitation.
FUNDINGThe RETAKO registry website has received funding from Astra Zeneca.
CONFLICTS OF INTERESTNone declared.
- –
Tako-tsubo syndrome is a potentially serious disease during its acute phase, associated with a relatively high rate of possible complications that result in notable in-hospital morbidity and mortality.
- –
There is a well established difference by sex in the appearance of TTS, with a female-to-male patient ratio of 9:1.
- –
The pattern of complications differed greatly between women and men with TTS. The overall prognosis was worse in men, who showed worse hemodynamic deterioration and had a higher rate of in-hospital mortality. Nevertheless, dynamic LVOT obstruction was a TTS complication found only in women, and female TTS patients also had a higher incidence of functional mitral regurgitation.
.
We would like to thank all the investigators participating in the RETAKO registry and the Spanish Society of Cardiology for its continued support for the development of this registry.