To the Editor,
Primary cardiac tumors are uncommon (0.001%-0.03%). The majority are benign (90%), with leiomyosarcoma accounting for 0.019% of the total.1 The tumor derives from smooth muscle cells and is characterized by high invasive capacity and thus, has often extended when the diagnosis is made.
We describe a 35-year-old woman who went to the emergency room for fever, asthenia, and anorexia of 2 months' evolution, with facial and upper thorax edema in the morning in the last weeks. The physical examination disclosed swelling of the eyelids, face, and upper chest, as well as inframammary collateral circulation.
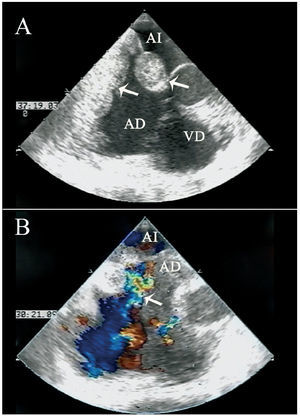
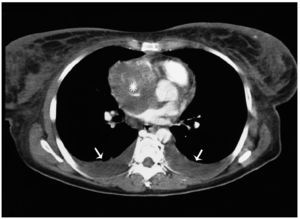
Transthoracic and transesophageal echocardiography showed a large mass of lobulated contours, 7.5×6 cm, that grew from the interatrial septum, in particular toward the right atrium, and occupied practically the entire atrial chamber at the top; growth toward the left atrium was minimal, and the fossa ovalis was preserved (Figure 1A). As a result, there was considerable obstruction of the superior vena cava flow, at its origin in the atrium, but without vascular wall infiltration (Figure 1B). Chest and abdominal contrast CT revealed a hypodense mass of irregular morphology in the right atrium that extended toward the left atrium and at the origin of both cava, without observing thrombosis (Figure 2). There was also mild pericardial effusion and collateral circulation to the azygos and hemiazygos system. The lymph nodes and mediastinal fat had an increased density consistent with lymphatic ectasia.

Figure 1. Transesophageal echocardiography, mid-esophageal view. A: at 20o, a large mass is seen in the atrium; the interatrial septum and a preserved fossa ovalis are evident (arrows). B: color Doppler ultrasound depicts compromised superior vena cava flow (arrow) at 70o. Blood stasis is observed in the atrial chamber. RA indicates right atrium; LA, left atrium; RV, right ventricle.

Figure 2. Contrast-enhanced chest computed tomography image shows a hypodense mass occupying virtually the entire right atrial chamber (*). Bilateral pleural effusion (arrows).
Surgery was performed, consisting of intraoperative biopsy of the right atrial free wall that confirmed the malignancy of the mass, and cavopulmonary connection was performed using a Goretex® ringed graft with a diameter of 8 mm. Specimens were taken for the pathological and immunohistochemical study, and the atrial free wall was reinforced with a bovine pericardium patch.
The anatomical pathology analysis revealed fusiform cells with considerable nuclear pleomorphism and mitotic activity. The immunohistochemical study was positive, mainly with actin, confirming a smooth muscle origin, and CD-34, indicating the vascular variety. The final diagnosis was vascular leiomyosarcoma.
The patient decided to go to her place of origin to start chemotherapy; subsequent contact with her relatives confirmed death after disease progression.
Leiomyosarcoma accounts for only a minor percentage of cardiac tumors1; 76% are located in the left atrium, 16% in the right atrium, and 8% in the ventricles.2 This type of tumor is extremely aggressive, with a high capacity for infiltration of adjacent tissues and extension to other organs. Onset is usually in the fourth decade, with a late, variable clinical presentation, as the symptoms tend to result from obliteration of the cardiac chambers and obstruction of the large vessels or valves.3
Histologically, the tumor consists of elongated cells with nuclei of smooth contours. The cytoplasm is eosinophilic and there are often abundant myofibrillae with no transversal striations. The nuclei may be large and vesicular or hyperchromatic and show frequent mitosis. Ultrastructurally, tumor cells detected by reticulin stain have numerous cytoplasmic filaments and a thick basal lamina. The immunohistochemical analysis is positive to vimentin, actin, myosin, desmin, laminin, and S-100 polyclonal antibody.3
Transthoracic and transesophageal echocardiography, CT scan, and magnetic resonance imaging make it possible to perform an initial diagnosis, assess the tumor extension, and, occasionally, differentiate the nature of the mass. Transesophageal echocardiography-guided transvenous biopsy allows histological diagnosis prior to surgery.4
There is no consensus regarding the therapeutic approach. The best strategy is radical surgery, although this may not always be possible because the tumor is too advanced, as occurred in our case. Therefore, surgery is usually done only for palliative purposes. On many occasions, despite complete removal, there is early recurrence of the disease.4 The benefit of postoperative adjunct therapy is inconclusive, although the survival prognosis has been improved in some cases.5,6 In particular, chemotherapy with doxorubicin, ifosfamide, etoposide, and vincristine appears to prolong survival, although there are no conclusive studies. Survival is around 12 months, but may be as high as 24 months if complete resection is achieved.3 The presence of high mitotic activity and necrosis, as well as right chamber origin,4 are adverse prognostic factors.