Keywords
INTRODUCTION
As in previous years and for over 2 decades now, one of the main tasks of the Board of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology is to collect and analyze data from Spanish hospitals engaging in these activities. The quality of the information obtained by the Working Group has improved year over year. 1-18 The data for 2009 were presented to members of the Working Group at its Annual Meeting, which was held from 17th to 19th June in Sitges. The data can also be found on the Working Group's website (http://www. hemodinamica.com).
The information obtained provides a picture of the current situation in Spain as well as allowing for comparisons with other countries. It also provides a means of evaluating and comparing the development of interventional cardiology across Spain's autonomous regions. The data is made freely available to extend knowledge of the way resources are distributed and illustrate trends in the use of diagnostic and therapeutic procedures.
Two aspects are of particular interest this year. First, there has been a significant increase in interventional activity in myocardial infarction (AMI), particularly in terms of the number of primary angioplasties; this is in line the European Society of Cardiology's 'Stent for Life' initiative.19 The aim of this initiative is to increase the percentage of AMI patients with ST segment elevation in which this type of revascularization is performed and Spain was one of the target countries for the initiative.20 The second aspect of interest is the continued increase in the percutaneous implantation of aortic valves, which is now carried out in almost all of Spain's autonomous regions.
This paper presents the nineteenth report on interventional cardiology activity in Spain and covers public centers as well as the majority of private centers.
METHODS
Data was collected on diagnostic and interventional cardiac activity in the majority of Spanish centers. Data collection was voluntary and no audit is performed though researchers submitting very inconsistent data are required to re-assess it. Data is collected using a standard questionnaire which is distributed to all catheterization laboratories in the country in two ways: on paper, and as an electronic form provided via the website of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (http://www.hemodinamica.com). The latter can be completed online. Paper versions are distributed and collected by the Izasa company. The data obtained was analyzed by the Board of the Working Group and is made public in this article.
For national and regional population-level calculations, the National Institute of Statistics' (NIS) estimates for January 1, 2009 were used, as published on the NIS website (http:// www.ine. es). The Spanish population stood at 46 157 222 inhabitants.
As in previous records, centers were defined as public, independently of its source of funding, if they served a certain population area within the public health system. All other centers were considered to be private.
RESULTS
Infrastructure and Resources
A total of 126 hospitals performing interventional activity in adults participated in the present registry. Of these, 9 also performed interventions in pediatric patients (Appendix 1). All of the public centers (74 hospitals) and 52 private centers (5 fewer than last year; it should be noted here that the registry does not include all of the private institutions carrying out interventional activity) submitted their data. Almost all of the centers performing interventional activity in Spain are therefore represented. The centers included provided a total of 178 catheterization laboratories, of which 112 (62%) were located in public health centers. A 24 hour emergency team was available in 73% of public centers and 75% of the private centers; 65% of the centers performed cardiac surgery.
The 126 participating centers reported that 432 doctors performed interventional activity during 2009, giving a distribution of 3.42 professionals per center. In public hospitals (321 physicians), there were 4.4 physicians per center and 3.48 per laboratory. In the private centers, there were 2 physicians per center and 2 per laboratory. Data was received from all centers regarding the availability of nursing staff. In total, centers employed 553 registered nurses (RN) and 107 radiology technicians (RT), giving an average of 5.2 RNs / RTs per center.
Diagnostic Activity
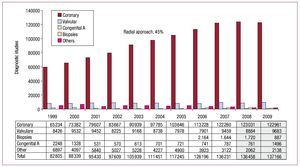
A total of 137 166 diagnostic procedures were performed in 2009. This represents only a minimal increase (<1%) over the previous year but is to be expected as the number of centers or laboratories in public hospitals, where most activity takes place, remained virtually unchanged. Of the diagnostic procedures reported, 122 961 were coronary angiograms, meaning there was no increase over 2008; 22% of the procedures were performed in women and 21% in patients aged over 75 years. These figures were similar to the previous year and give a national average of 2664 coronary procedures per million inhabitants. That figure is virtually unchanged from 2008 and is still substantially below the 2005 European average of 4030 coronary angiograms per million inhabitants in countries participating in the Registry.21
Figure 1 shows the distribution of all diagnostic procedures since 1999.

Figure 1. Evolution of the number and type of diagnostic studies conducted between 1999 and 2009.
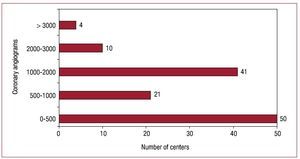
In 2009, as in 2008, public centers performed 85% of diagnostic activity, with 55 centers performing over 1000 coronary angiograms, and 14 of them, over 2000 (Figure 2). Centers performed an average of 1,088 diagnostic procedures (770 per laboratory), so again were essentially unchanged from the previous 2 registries.14-18 Seventeen hospitals performed fewer than 1000 coronary angiograms.

Figure 2. Distribution of centers according to the number of coronary angiograms.
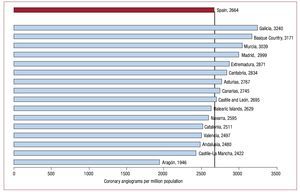
As mentioned in the introduction, the national average was 2664 coronary angiograms per million inhabitants. Distribution by regions is shown in Figure 3. Apart from the region at the lowest end of the scale, the difference between the region with highest rate and that with the second to lowest rate was only 818.

Figure 3. Distribution of coronary angiograms per million population and region.
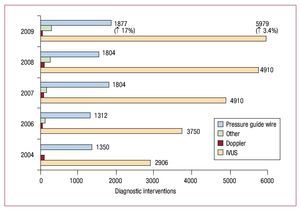
With regard to intracoronary diagnostic techniques, intravascular ultrasound was the most frequently used technique, followed by the pressure guide wire. With respect to previous years, there was some stagnation in the use of intravascular ultrasound (only a 3.4% increase in use compared to 2008), while the use of pressure guide wires increased by 17.7% (its use declined 14% in the previous year). Use of optical coherence tomography continued to increase, to a total of 327 interventions, representing an increase of 17% over 2008. On the other hand, use of the intracoronary Doppler guide wire decreased drastically, by 49.5%, to a total of only 52 cases. Figure 4 shows the evolution of intracoronary diagnostic techniques in recent years.

Figure 4. Evolution of intracoronary diagnostic techniques. IVUS: intravascular ultrasound.
As regards accessory pathways, the increased use of the radial artery seen in previous years was maintained, and approached parity with the femoral artery. It was used in 45% of cases in 2009, compared to 48% in 2008 and 41.7% in 2007.
Coronary Interventions
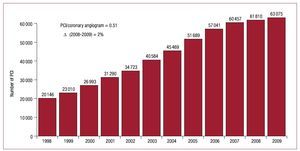
The increase in percutaneous coronary interventions (PCI) was virtually identical to the previous year (2%), with the number in 2009 standing at 63 075. The historical development of the intervention in Spain is shown in Figure 5. The number of PCIs per million inhabitants was 1391, a slight increase over the previous year (1%) but still well below the latest published European figures, with a rate of 1601 PCIs per million inhabitants in 2005.18 90% of coronary interventions were performed in National Health Service centers.

Figure 5. Evolution in number of percutaneous coronary interventions (PCI) between 1998 and 2009.
The PCI / angiography ratio was 0.51 in 2009, which represented a slight increase over 2008. This reflected the larger increase in the number of PCIs compared to coronary angiograms. The number of procedures for multivessel disease fell by 2.2% over the year and represented 24.8% of the total number of PCIs. The frequency of ad hoc procedures performed during diagnosis also remained unchanged at 76% (47 902).
Distribution by sex and age was very similar to 2008 with 19.8% of procedures performed in women (compared to 18.9% the previous year) and 23.3% of procedures performed in patients over 75 years of age (compared to 20% in 2008). In 5.6% of cases, PCI was performed on one or more restenotic lesions (5.2% in 2008). The number of interventions for restenotic lesions has been relatively stable for almost 5 years a fact which may be explained, at least in part, by the lack of any real increase in stent use over that period.
The significant increase in unprotected interventions in the common arterial trunk (CAT) is also noteworthy. The figure increased to 1973 operations, up 19% over the previous year, and representing 3.12% of total PCIs.
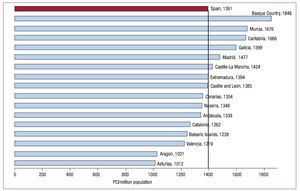
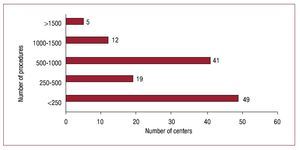
Glycoprotein IIb / IIIa (GPIIb / IIIa) inhibitors and adjunctive antithrombotic drug therapy were used in 14,376 procedures (22.8%): 65.3% with abciximab, 11.5% with tirofiban, 7.1% with eptifibatide, and 16% with bivalirudin. These figures represented an increase of almost 50% over the previous year. They refer to all procedures using antiGPIIb / IIIa; the time of drug administration is not specified, as this variable is not included in the data collection form.The breakdown by regions for the 1391 PCIs per million inhabitants in Spain is shown in Figure 6. Regional distribution was similar to 2008 (836), although if the first and last two regions are excluded, levels were similar to those for 2007 and prior years (453). Figure 7 shows the distribution by centers. As can be seen, 58 centers performed over 500 PCIs throughout the year (46%), and 17 centers could be classified as high-volume (>1000).

Figure 6. Distribution of percutaneous coronary interventions (PCI) per million population and region.

Figure 7. Distribution of centers according to the number of percutaneous coronary interventions performed in 2009.
Intracoronary diagnostic techniques (echocardiography, intracoronary ultrasound [IVUS] and pressure guide wire), which are used primarily to assess the severity of intermediate lesions or the result of the intervention, were similar in number to 2008, with IVUS and pressure guide wires representing 9.4% and 2.9% of total PCIs, respectively.
Radial access in coronary interventions increased slightly to 45.5% and, for the first time, reached similar proportions to its use in diagnosis (45%). As regards femoral access, vascular closure was used in 40,450 cases, 10% more than last year. Collagen was used in 66.7% of cases, compared to suture in 19.3%. Other devices were used in 14% of cases.
Stents
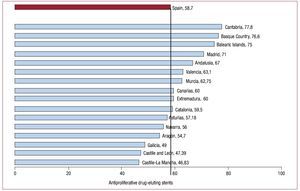
A stent was implanted in 94.8% of all coronary interventional procedures in 2009 (essentially the same proportion as in 2008), with a total of 102 850 units used in 59 834 PCIs. The mean number of stents per patient decreased to 1.63 (compared to 1.76 in 2008), which may be in part due to the increase in primary angioplasty in AMI compared with electives. The use of drug-eluting stents (DES) was almost identical to 2008 (58.7%), with 60,468 units employed. Use of a DES alone, as opposed to a bare metal stent alone or the two types of stent together, represented only 33.6% of the total number of procedures, almost 20% less than in 2008.
The use of DES varied substantially between regions and ranged from 77.8% in Cantabria to 46.8% in Castile-La Mancha (Figure 8).

Figure 8. Distribution of antiproliferative drug-eluting stents as a percentage of total stents implanted by region.
Other Devices and Percutaneous Coronary Intervention Procedures
Use of rotational atherectomy continued to increase over the previous year, albeit discreetly (5.3%). There was no report of any directional atherectomy procedure or intracoronary brachytherapy. Among other devices, use of a cutting balloon increased dramatically (33%), to 1,784 procedures. The same was true for the thrombectomy catheter, which grew from 4427 cases in 2008 to 5481 in 2009.
Intervention in Acute Myocardial Infarction
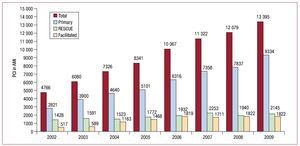
A total of 13 395 procedures were performed in the context of AMI (21.2% of all PCI), an increase of 10% over 2008. Of those, 17.3% were performed in women (identical to 2008) and 21.5% were performed in individuals over 75 years of age, 1.5% more than in the prior year.
Among the range of PCI procedures performed in the acute phase of AMI, there was a marked increase in primary angioplasty, which increased from 7837 procedures in 2008 to 9334 in 2009 (up 19%). A large part of this increase could be due to the incorporation of the metropolitan area of Barcelona, with more than 5 million inhabitants, within a primary angioplasty program which commenced in June 2009. Primary angioplasty accounted for some 15% of angioplasties and 65% of all infarct PCIs; 1916 (14.5%) were facilitated PCIs and 2145 (19.9%) were rescue PCIs (Figure 9).

Figure 9. Evolution in the types of percutaneous coronary interventions (PCI) in acute myocardial infarction (AMI).
National data on the total number of AMIs with ST elevation (STEMI) are not available, but given an annual estimate for Spain of 45 000 STEMI,22,23 primary PCI would be used in only 20% of cases, whereas the 'Stent for Life' initiative recommends a target of 70% of primary PCIs in AMI.19
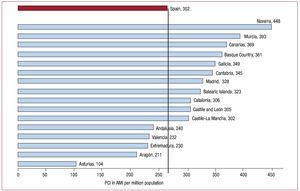
Nationwide distribution of PCIs in AMI shows a similar pattern to that observed in 2008, whereby autonomous communities with a continuous care program for AMI had the best data (Figures 10 and 11).

Figure 10. Distribution of percutaneous interventions (PCI) in acute myocardial infarction (AMI) per million population and region.

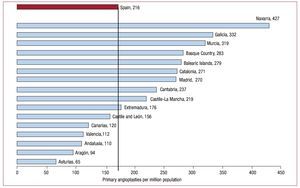
Figure 11. Distribution of primary angioplasty per million population and regions.
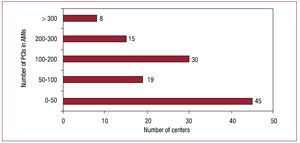
In terms of the number of procedures per center, only 23 performed over 200 angioplasties in AMI throughout the year, while 45 centers performed fewer than 50 (Figure 12).

Figure 12. Distribution of centers according to the number of percutaneous coronary interventions (PCI) in the context of acute myocardial infarction (AMI).
Non-Coronary Interventions in Adults
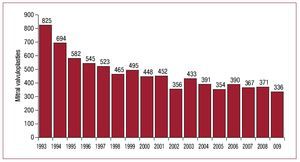
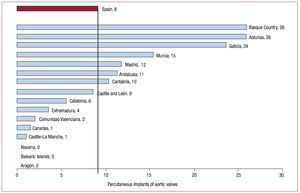
Mitral valve replacement remained the most frequent non-coronary intervention (336 cases), with figures that were very similar to those of recent years. Outcomes were also the same as the previous year, with a success rate of 96% and major complications in 2% of procedures (Figure 13). Aortic valve replacement continued to increase, from 75 in 2008 to 134 in 2009. The growth in percutaneous aortic valve implantation was spectacular, from 151 cases in 2008 to 426 cases in 2009. Of these, 224 were self-expanding (94% success, with hospital mortality of 5.8%) and 202 used expandable balloons (90.5% success, with hospital mortality of 9.4%). The breakdown by regions is shown in Figure 14.

Figure 13. Evolution of mitral valvuloplasties in Spain.

Figure 14. Distribution of percutaneous aortic valve implantation by region.
The treatment of adult congenital heart disease continued to be the most common non-coronary interventional procedure in the current registry, with 731 procedures performed (up from 635 in 2008). The most frequent of these was atrial septal defect (ASD) closure, with a total of 329 cases and a 96% success rate. Of the cases treated, 2% had complications, including device embolization or tamponade. Procedure mortality was zero, as in 2006, 2007 and 2008. Closure of the foramen ovale was performed in 232 cases, with a success rate of 98%, and 37 aortic coarctations were performed (14 more than the previous year). Other procedures performed included closure of ductus, ventricular septal defects, and fistula.
In all, 92 paravalvular leaks were treated, almost double the number treated in 2008; 66 were mitral and 26 aortic.
Interventions in Pediatric Patients
Ten centers provided data on their activity in pediatric age patients (16 years of age or under). These included 84 CIA closures and 52 ductus closures, 134 aortic valvuloplasties, 37 treatments for aortic coarctation, and 33 lung valvuloplasties.
CONCLUSIONS
The 2009 Registry indicates that we have generally reached a plateau in the evolution of diagnostic and therapeutic procedures, though it is also true that angioplasty in the context of AMI, particularly primary angioplasty, has grown considerably, possibly because of the incorporation of new regions such as Catalonia into 'open' primary percutaneous transluminal coronary angioplasty (PTCA) programs. We believe that in subsequent years, given that there is no apparent increase in the number of public centers or operating theatres, any growth in the number of coronary interventions will come through primary angioplasty. This is now a focus for our working group, in parallel with the Spanish and European Cardiology Societies, the aim being to expand the 'Stent for Life' program to as many autonomous regions as possible.
Diagnostic activity in general was also very similar to the previous year, with a moderate increase in the use of intravascular ultrasound and a slightly larger increase in the case of the pressure guide wire.
Variations between the regions were maintained as regards PCI in general and, in particular, for myocardial infarction.
The use of ADES increased by only 0.5% compared to 2008, to a national average of 58.7%, with considerable variety between regions and a similar distribution to that observed in previous Registries. The use of rotational atherectomy grew by only a small amount compared to growth recorded in the previous year (5.3% compared to 30.6%).
The radial accessory pathway was used in almost 50% of cases, both for diagnosis and in interventions and is used increasingly in the acute phase of stroke.
Moving beyond coronary interventions, percutaneous aortic valve implantation showed the strongest growth among all of the parameters examined, from 151 in 2008 to 426 in 2009. Of course, it may not be possible to maintain these levels of growth due to the economic situation in Spain and the high cost of these devices.
We would like to end by announcing the launch of a specific registry of percutaneous aortic valves and our intention to set up, as soon as possible, another registry of activity based on individual patient data.
ACKNOWLEDGMENTS
The Board of the Working Group on Cardiac Catheterization and Interventional Cardiology would like to thank the directors and staff of Spain's catheterization laboratories, and those responsible for data collection, for all the work which has made this Registry possible.

ABBREVIATIONS
AMI: acute myocardial infarction
PCI: percutaneous coronary interventions
DES: drug-eluting stent
CAT: common arterial trunk
IVUS: intracoronary ultrasound
STEMI: ST-elevation acute myocardial infarction ASD: atrial septal defect
PTCA: percutaneous transluminal coronary angioplasty
ADES: antiproliferative drug-eluting stents
Correspondence: Dr. J.F. Díaz.
Unidad de Hemodinámica. Hospital Juan Ramón Jiménez. Ronda Norte, s/n. 21005 Huelva. Spain
E-mail: JFDIAZF@telefonica.net