
Keywords
INTRODUCTION
Deaths caused by cardiovascular disease continue to be one of the major concerns for both industrialized and developing nations.1 Various longitudinal studies have shown that the cardiovascular risk factors such as hypertension, dyslipidaemias, and insulin-resistance begin in infancy and continue through to adulthood.2,3 Furthermore, the levels of cardiovascular risk in children and adolescents have increased over recent years, with the majority of studies associating this with the prevalence of obesity which has reached pandemic levels.4 Therefore, the prevention of infant obesity has become a priority in public health policies in many countries.5
Physical activity and diet have been shown to be the main factors in the prevention of cardiovascular illnesses and obesity.6 However, recently sedentary behaviour has begun to be shown as having an important role in the development and prevention of these diseases, and indications have also been made that physical activity and sedentary behaviour are not opposing sides of the problem.7,8 Recent studies that have attempted to evaluate how sedentary lifestyles are related with obesity and cardiovascular risk factors in children and adolescents have found contradictory results.9-16 The majority of these studies have measured sedentary behaviour with the use of questionnaires, collecting information about different behaviours such as time spent watching the television, using the computer or playing videogames. However, various studies have shown that the time spent doing these sorts of activities only makes up a small part of the day taken up by sedentary behaviour.17,18 At present, the key instruments for assessing physical activity, such as accelerometers, allow for much more precise measurement to be taken of the exact time spent engaged in activities of varying intensity. Consequently, accelerometers can measure the time that children and adolescents spend engaged in sedentary activities and not only the time spent engaged in technological pass-times.7,8
Therefore, the main aim of this study is to examine the associations between the time spent in sedentary behaviour by objectively measuring the different cardiovascular risk factors in adolescents. Furthermore, the study also aims to evaluate how general and abdominal adiposity are associated with the cardiovascular risk factors in this age group.
METHODS
Participants
The adolescents selected for this study participated in the AFINOS study (La Actividad Física como Agente Preventivo del Desarrollo de Sobrepeso, Obesidad, Alergias, Infecciones y Factores de Riesgo Cardiovascular en adolescentes, Physical Activity as a Preventative Agent of the Development of Overweight, Obesity, Allergies, Infections, and Cardiovascular Risk Factors in Adolescents). Using a questionnaire, this study assessed the state of health and a selection of lifestyle indicators in a representative sample of adolescents from Madrid aged between 13 and 17 (≈2000). In a subgroup of 232 adolescents, blood parameters were also assessed and a more exhaustive health and lifestyle assessment was carried out. From this subgroup 201 adolescents (99 females) showed valid data from the accelerometer, anthropometric and blood parameter assessments, and were consequently used in this study. Data collection was carried out in 2007-2008.
Before starting the study, adolescents and their parents/guardians were informed of the study characteristics and were asked to sign an informed consent form. The AFINOS study was approved by the Ethical Committee of the Hospital Puerta de Hierro in Madrid, and the Bioethical Committee of the Spanish National Research Council.
Physical Examination
This study used the anthropometric protocol as standardized in the AVENA study.19 Skinfolds were measured on the left hand side of the body using Holtain calipers to obtain the measurements of the following: triceps, biceps, subscapula, suprailiac, thigh, and calf. The body perimeters were measured using an extendible metric measuring tape and the following 5 areas were measured: biceps, contracted biceps, waist, hips, and thigh. Weight and height were measured using standard procedures. Body mass index was calculated as weight/size2 (kg/ m2). In this study the sum of the 6 skinfolds was used as an indicator of general adiposity and the perimeter of the waist was used as an indicator of abdominal adiposity. The developmental stage of the participants was assessed in accordance with the Tanner and Whitehouse system.20
Sedentary Behaviour
The time spent in sedentary activities is assessed objectively using the ActiGraph GT1M accelerometer. This is a small, light, compact device which measures vertical acceleration in ranges of 0.05-2 G with a response frequency of 0.25-2.5 Hz. The ActiGraph Accelerometer has been extensively validated for its use with these age groups.21 The movements (known as counts) captured by the accelerometer are added together to achieve a specific time interval.
The processes and results obtained using the accelerometer in the AFINOS study for assessing physical activity have recently been published.22 In brief, adolescents wore the accelerometer at hip height, attached to their backs with an elastic belt for 7 days, and activity was registered every 15 seconds. During this time the participants could only remove the accelerometer to sleep or when taking part in water-based activities. Only adolescents with ≥4 valid days' results were included in this test which included at least 1 weekend day. A valid day was considered to be one in which the adolescent wore the accelerometer for at least 10 hours. For the purposes of calculations, groups of 10 minutes with continuous zeros were excluded. The time engaged in sedentary activities was recorded as the time in which the level of activity was <100 counts per minute.
Cardiovascular Risk Factors
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured using the Omrom M6 (mm Hg) digital tensiometer. This tensiometer has been validated for use in accordance with European Hypertension Society protocols.23 Mean blood pressure (MBP) is calculated as DBP+1/3´(SBPDBP).
Blood testing was carried out between 8 AM and 9 AM after fasting for at least 10 hours. For all participants blood was taken from the cubital vein using a needle and was collected in a tube with EDTA, a tube with heparin and a tube with dry gel for saline solution. The levels of triglycerides (TG), total cholesterol (TC), cholesterol linked to high density lipoproteins (HDL-C) and glucose were measured using colorimetric enzymatic methods using an AU2700 Olympus analyser. The fraction of cholesterol linked to low density lipoproteins (LDL-C) was calculated using the Friedewald formula.24 The apolipoprotein A-1 (Apo-A1) and B-100 (Apo-B100) were obtained using the turbidimetric method with Olympus AU2700 analysing equipment.
Cardiovascular Risk Index
A cardiovascular risk index was calculated using the values of MBP, HDL-C, TG, and glucose. These variables were chosen to create the index because they are included in the definition of the metabolic system in adults25 and youngsters.26 As the definition of the metabolic system uses SBP and DBP to determine the risk of hypertension, the indicator uses MBP which includes both variables. In order to create the index, each factor was initially standardised using the regression of the results for age, gender, developmental stage, and tobacco consumption (daily, occasionally, ex-smoker, non-smoker) values, using a lineal regression process.3 The HDL-C value was then multiplied by -1 as this is inversely related to cardiovascular risk and finally, the standardised remainders (z-score) of the 4 variables were added together. The higher the value in the cardiovascular risk index, the higher the cardiovascular risk.
Statistical Analysis
The results are presented as mean (standard deviation). Normality was assessed for all the variables and in those cases in which a normal distribution was not seen, a logarithmic transformation was carried out (ln). The differences between genders was analysed using simple analysis of variance (ANOVA), except for the time spent engaged in sedentary behaviour which was analysed using analysis of covariance (ANCOVA), adjusting it by the valid daily time during which the accelerometer was worn. No significant interactions were seen between gender and the other variables used in the study so the analysis for boys and girls was carried out together to achieve better statistical strength.
The associations between the time spent doing sedentary activities and adiposity with the factors of cardiovascular risk (SBP, DBP, MBP, CT, TG, HDL-C, LDL-C, glucose, Apo-A1, and Apo-B100) were assessed using ANCOVA dividing the sample according to the sedentary behaviour level (low, average, high) and the levels (low, high) of general adiposity (sum of 6 skinfolds) and abdominal adiposity (perimeter of waist) adjusting the differences for age, sex, developmental stage, and tobacco intake. The associations of sedentary behaviour and adiposity with the cardiovascular risk index were assessed using ANOVA. In this case, there were no adjustments made as this index was previously standardized for the confounding variables.
The combined influence of sedentary behaviour and the level of adiposity in the cardiovascular risk index was analysed by dividing the sample into 6 groups (2 groups for adiposity ´ 3 groups for sedentary behaviour), obtaining the differences between the groups using ANOVA. The differences between the median of each group was analyzed using the Bonferroni correction for multiple comparisons. All the analyses were carried out using the SPSS v.15 program for Windows. The level of statistical significance was established in P<.05.
RESULTS
The descriptive characteristics for the adolescents are presented in Table 1. The ANOVA analysis showed that females had generally higher levels of adiposity than males, whilst males had higher levels of abdominal obesity. With cardiovascular risk factors, males had higher SBP, MBP and glucose levels than females, whilst females showed higher levels of HDL-C and Apo-A1. No significant differences were found between sexes for the cardiovascular risk index nor for the daily amount of time spent engaged in sedentary behaviour.

The differences in cardiovascular risk factors according to the level of sedentary behaviour (low, average, high) are presented in Table 2. The ANCOVA analysis adjusted by the confounding variables showed significant differences between the groups of adolescents in the levels of SBP, TG and glucose, and similarities in the levels of MBP (P=.077) and HDL-C (P=.066). In general, the adolescents that spent more time engaged in sedentary activities had higher levels of SBP, TG, and glucose than the adolescents that spent less time engaged in sedentary behaviour. The ANOVA analysis showed significant differences (P=.037) in the cardiovascular risk index between tertiles of sedentary behaviour, also observing that the adolescents who spent more time engaged in sedentary behaviour had a higher cardiovascular risk than those which spent less time involved in such activities. There were no significant differences in the degree of general adiposity and abdominal adiposity between the 3 tertiles of sedentary behaviour.

Table 3 shows the differences in cardiovascular risk according to the level of general and abdominal adiposity. The ANCOVA analysis showed how adolescents with a higher level of general adiposity have higher levels of DBP, LDL-C, CT, and Apo-B100. Furthermore, adolescents with higher abdominal adiposity have higher levels of SBP, MBP, LDL-C, CT, TG, and Apo-B100, and lower levels of HDL-C. The ANOVA analysis also showed a higher level of cardiovascular risk in adolescents with a higher level of general and abdominal adiposity (P<.001, in both).

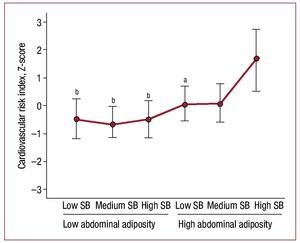
Upon dividing the sample into 2 groups according to the level of general adiposity (low and high), and into 3 groups according to the time spent engaged in sedentary behaviour (low, medium, high), significant differences were seen (F=6.318; P<.001) in the cardiovascular risk index value (Figure 1). Similarly, when the sample was divided into 2 groups in keeping with the abdominal perimeter measurement (low, high) and 3 groups according to the time spent engaged in sedentary behaviour, significant differences were also observed (F=4.899; P<.001) in the cardiovascular risk index value (Figure 2). In both sets of analysis it was seen that amongst the adolescents with higher general abdominal adiposity the ones that spent less time engaged in sedentary behaviour had a lower cardiovascular risk than those that spent more time engaged in that sort of behaviour.

Figure 1. Combined influence of general adiposity (sum of 6 skinfolds) and the time spent engaged in sedentary behaviour over cardiovascular risk in adolescents. SB indicates sedentary behaviour. The significant differences express with regards the group with a high level of sedentary behaviour and general adiposity. The error bars represent a typical error in the measuring. aP<.05. bP<.01. cP<.001.

Figure 2. Combined influence of abdominal adiposity (perimeter of waist) and the time spent involved in sedentary behaviour over cardiovascular risk in adolescents. The significant differences express with regards the group with high levels of SB and abdominal obesity. The error bars represent a typical error in the measuring. SB indicates sedentary behaviour. aP<.05. bP<.01.
DISCUSSION
The main results from this study show that the amount of time that the adolescents spent involved in sedentary behaviour on a daily basis is associatedwith higher cardiovascular risk. Consequently, the adolescents who were more sedentary on a daily basis showed higher levels in some of the risk factors that were analysed (SBP, TG, and glucose) as well as worse values in the cardiovascular risk index that was employed.
The majority of studies carried out on children and adolescents have valued the time engaged in sedentary activities with the use of questionnaires, asking such things as how much time is spent watching television.17,18 Although the time spent watching television can represent an important part of the time that young people spend engaged in low intensity activities, it is a long way from being a good indicator of the daily amount of time spent involved in sedentary activities overall. In addition to this, the assessment of these sedentary patterns via the use of questionnaires with these age groups has certain limitations.27 Furthermore, the time spent watching television is associated with unhealthy eating28 and sleeping29 patterns, a phenomenon that can distort some of the associations found between watching television and different health indicators. All the elements reviewed could contribute to the explanation of the ambiguous results present in available literature regarding the contribution of sedentary behaviour to the development of obesity9-12 and diverse factors of cardiovascular risk.13-16
Hamillton et al7 suggested the possibility that time spent involved in sedentary activities (physiological inactivity or "time spent sitting down"), may be a relevant element in the development of obesity, cardiovascular and metabolic diseases and even some types of cancer. Pate et al8 have brought up the possibility of objectively assessing the daily amount of time spent engaged in low levels of physical activity using an accelerometer to examine the ideas put forward by Hamillton et al.7 Consequently, the first studies have recently been published by Healy et al,30,31 which have found that in Australian adults there are associations with diverse cardiovascular risk factors.
In children and adolescents, the majority of studies have been carried out under the framework of the European Youth Heart Study (EYHS). Ekelund et al,32 found that in a group of 1709 children and adolescents there were positive associations between the time spent engaged in sedentary behaviour and diverse cardiovascular risk factors (SBP, DBP, glucose, TG, insulin) as well as each index that assessed the combination of cardiovascular risk and metabolic syndrome.
In another sample from the EYHS study, Rizzo et al33 did not find associations between the time spent engaged in sedentary behaviour and three markers of insulin resistance (glucose, insulin, insulin-resistance, or HOMA). However, Sardinha et al34 did find a link between the Portuguese sample of the EYHS study and HOMA, regardless of the level of general and abdominal adiposity. A study of children between the ages of 3 and 8 did not find an association between time spent in sedentary behaviour and blood pressure, although they did find a link with the time spent watching television.35
The results obtained in our study indicate that the time spent in sedentary activities can play an important role in the development of cardiovascular risk during adolescence, although it did not find any associations between sedentary lifestyle and obesity. These results suggest the need to keep in mind a reduction in sedentary behaviour as an additional strategy in the prevention of the premature development of cardiovascular risk in infancy and adolescence, as well as the promotion of physical activity and improvements to eating habits.
Some organizations have proposed recommendations regarding the limitation of sedentary behaviour in children and adolescents. However, these recommendations often refer exclusively to "screen time" (television + computer/ videogames). The American Academy of Paediatrics suggests that young people should spend no longer than 2 hours a day in front of a screen.36 However, the periods of inactivity in children and adolescents can be much longer than just the time spent engaged in "screen time" type activities as has been mentioned earlier. The results of our study suggest the need for carrying out recommendations regarding a reduction in the total amount of time that children and adolescents spend inactive, and not only a reduction in screen time. The recommendations from Corbin and Pangrazi37 consider this aspect and they show that periods of inactivity over 2 hours a day should be avoided in children and activities. Although this recommendation has not been researched, some recent adult data suggests that interruption of long periods of inactivity can be related with a better metabolic profile.38 To our knowledge, one intervention study known as TAKE10! (www. take10.net) is specifically directed towards breaking up long periods of inactivity that are regularly found in boys and girls during the school day, introducing short periods of 10 minutes of moderate to vigorous activity between academic activities. The preliminary results from this study have been positive.39
An additional objective of our study has been the assessment of the degree of association between various indicators of adiposity and cardiovascular risk. To this end, the differences have been assessed in groups according to their level of adiposity using the sum of 6 skinfolds and waist perimeter as indicators of general adiposity and abdominal adiposity respectively. The results have shown how the group with a higher level of general adiposity have less favourable results in 5 of the 11 cardiovascular risk factors assessed, whilst the group with more abdominal fat showed less favourable results in 8 of the 11 factors. Both results confirm the relevance of obesity and in particular abdominal fat, with regards the development of cardiovascular risk in adolescents.
The most commonly used definitions of metabolic syndrome in adults25 and children26 include abdominal obesity, assessed as a measurement of the perimeter of the waist, although there are other anthropometric variables that could be used. For example, the International Diabetes Federation uses the risk of an excess of waist perimeter as a criteria sine qua non to quantify whether metabolic syndrome exists or not during the paediatric age.26 Therefore, it is important to continue to work towards reducing infantile and juvenile obesity as a public health strategy.
Having found an association in our study between the time spent in sedentary behaviour and adiposity with cardiovascular risk, the study has tried to analyse the possible combined influence of both factors. The results show that adolescents with higher levels of adiposity and sedentary behaviour have a higher cardiovascular risk. This data suggests that an increase in sedentary behaviour increases cardiovascular risk in the more obese population. Earlier studies have also shown that a better physical state is associated with less cardiovascular and metabolic risk in obese children and adolescents ("obese on top form").40
The main limitations of this study are those inherent to its transversal study desing. However, the use of an accelerometer as a procedure for measuring the time spent by adolescents engaged in sedentary behaviour is a methodological component which reinforces the results found and is a further development with regards the bulk of previous research. The limitations with regards the use and assessment of the results obtained using the accelerometer in the AFINOS study have been previously reported.22
CONCLUSIONS
The results of this study suggest that the time that adolescents spend on a daily basis engaged in sedentary activities is related to higher cardiovascular risk. In addition to this, adolescents with less favourable adiposity and who spend more time engaged in sedentary behaviour tend to show higher cardiovascular risk.
ACKNOWLEDGMENTS
The authors would like to thank all the adolescents who took part in this study.

ABBREVIATIONS
Apo A-1: apolipoprotein A-1
Apo B-100: apolipoprotein B-100
DBP: diastolic blood pressure
HDL-C: high-density lipoprotein cholesterol
LDL-C: low-density lipoprotein cholesterol
MAP: mean arterial pressure
SBP: systolic blood pressure
TC: total cholesterol
TG: triglycerides
SEE ARTICLE ON PAGES 261-4
The Annex details the researchers and centres participating in the AFINOS study.
The AFINOS study is subsidized by the Spanish National R+D plan (Plan Nacional de I+D), which is part of the Strategic Sports and Physical Activity Action Group (DEP2006-56184-C03-02/PREV (Acción Estratégia de Deporte y Actividad Física) of the Spanish Ministry of Education and Science, and with assistance from AP2006-02464 from the Spanish Ministry of Education and Science.
Correspondence: Dr. O. L. Veiga.
Departamento de Educación Física, Deporte y Motricidad Humana. Universidad Autónoma de Madrid. Facultad de Formación de Profesorado y Educación. Campus de Canto Blanco.
Ctra. de Colmenar, Km 11. 28049. Madrid. Spain.
E-mail: oscar.veiga@uam.es
Received May 10, 2009.
Accepted for publication August 26, 2009.