
To the Editor,
The present article presents the case of a 70-year-old male, with a history of acute anterolateral myocardiac infarction (AMI) in 1986 and inferior AMI in 1992. Coronary arteriography was performed in 1995, which showed occlusion of the distal RCA and stenosis in 90% of the proximal LAD, with an ejection fraction (EF) of 29%. Balloon angioplasty was performed in the proximal LAD.
The patient was admitted to hospital in 2007 with unstable angina. Coronary arteriography (Figure 1) showed occlusion of the distal RCA, 90% ostial lesion in the Cx, absence of restensosis in the LAD, and an EF of 25%.

Figure 1. RCA with occlusion in the distal segment (left). Result of RCA angioplasty following implantation of 2 Xience stents in the distal RCA and a Cypher stent in the middle RCA with reverse collateral flow to the Cx (right).
On February 2, 2007 angioplasty of the distal RCA (acute occlusion which had developed over 15 years in the collateral, isolateral, and contralateral arteries) was attempted, followed by an angioplasty on the lesion originating in the Cx (protected by reverse flow in the collateral arteries from the RCA to the Cx). The patient was receiving treatment with acetylsalicylic acid, clopidogrel, tirofiban, and low molecular weight heparin.
A 7F JR4 guiding catheter was used (right femoral), as well as a 5F JL3.5 (left radial, to visualize the contralateral circulation from the left coronary artery). Since the 7F catheter did not provide sufficient support, a 5F JR4 one was used for the active catheterisation of the RCA. Following the administration of 8000 U of intracoronary heparin, an attempt to cross the lesion was made using Confianza Pro coronary guidewire (Asahi, Abott Vascular). The occlusion was crossed using an Avion OTW balloon (Invatec) and a Courier Microcatheter (Micrus Endovascular Corporation). Following a contralateral injection it was observed that the guidewire was located in false lumen and numerous failed attempts were made to move it to true lumen using the double-wire technique (Whisper guidewire, Abbott Laboratories; Pilot 50 Abbott Laboratories and Confianza Pro).
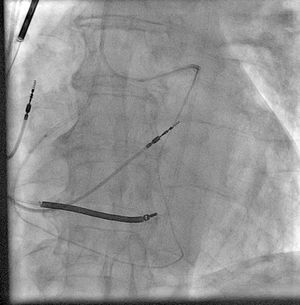
Given that it was not possible to enter the true lumen, a retrograde angioplasty was performed via a septal branch. A Whisper guidewire was passed through the aforementioned branch to the distal bed of the left anterior descending artery (LAD) and the Courier microcatheter was subsequently passed through to this level. The lesion was crossed from the LAD using PTC Graphix guidewire (Boston Scientific), which was entered retrogradely through the RCA to the interior of the guiding catheter located in the RCA. Since the guiding catheter used was 100 cm (the length of which prevented it from reaching the balloon retrogradely in the obstructed area), the guide was retrieved using a snare (Amplatz goose neck, EV3). This was entered via the catheter positioned in the RCA. An attempt was made to reveal the guide using the snare via the guiding catheter in the RCA. This required a great deal of force and resulted in deep intubation in the left artery. The guide was fixed onto the snare, thus giving sufficient support to move the microcatheter retrogradely up to the 5F guiding catheter located in the RCA (Figure 2). A BMW guidewire (Abbott Laboratories) was then passed from the proximal RCA and entered into the microcatheter. The guidewire was passed to the septal branch via the microcatheter and subsequently removed leaving the guidewire in the distal LAD. A 1.25×14 Avion ATW balloon was used to dilate the occlusion in the distal RCA. The balloon was inflated several times along the distal RCA and LAD and the occlusion of the posterolateral artery (PLA) was confirmed. A Whisper guidewire was passed through to the PLA and dilated using a 2×15 Maverick Balloon (Boston Scientific Corporation). Finally, 2 overlapping 2.5 x 28 Xience stents (Abbott Laboratories) were implanted in the PLA and distal RCA and the kissing balloon technique was used on the LAD and PLA. A 3×33 Cypher stent (Cordis Corporation) was implanted in the middle RCA, which presented dissection caused by the active intubation with the guiding catheter, with good angiography results (Figure 1, right) and reverse collateral flow towards the Cx. The peak creatine kinase was 305 U/L.

Figure 2. Microcatheter passed retrogradely, from the septal branch to the LAD and from here to the proximal RCA.
The following day angioplasty was performed in the Cx ostium with the implantation of a 3.5×12 metal Vision stent (Abbott Laboratories), with excellent results. The patient remained asymptomatic and was discharged after 24 hours.
The technique used was a modification of that used by Japanese authors for retrograde angioplasty. Since it was not possible to reach the lesion retrogradely using a balloon, via a normal length guiding catheter (sold in Europe), the guidewire was passed retrogradely up to the guiding catheter in the RCA. Since it was not possible to reveal the guidewire using the snare through the guiding catheter located in the RCA, the microcatheter was passed retrogradely up to the RCA, while tension was maintained in the guide using the snare (this could have been performed by inflating a balloon inside the guiding catheter in the RCA linked to the retrograde guide) and entering an anterograde guide through the tip of the microcatheter to complete the procedure using the conventional method.