To the Editor,
Heart resynchronization therapy (HRT) improves heart function, quality of life and survival in patients with symptomatic heart failure, QRS ≥120 ms and left ventricular dysfunction.1 More and more studies have shown benefit in patients with atrial fibrillation (AF), as long as biventricular stimulation rates greater than 90%2,3 are achieved. If this target is not achieved by pharmacological treatment, atrioventricular node ablation is indicated.
We present the case of a 66-year-old man suffering from hypertension, diabetes and dyslipidemia, diagnosed with ischaemic dilated cardiomyopathy with a LVEF of 30%, surgically revascularized, with AF and functional class NYHA II-III, with frequent hospitalizations due to heart failure decompensation, which led to the decision to implant an automatic implantable defibrillator with heart resynchronization therapy (HRT).
Stimulation rates of less than 80% were registered, so it was decided to perform His branch ablation by the arterial route, to avoid displacing the left ventricle electrode by manipulating the ablation catheter near the coronary sinus. The patient suffered from severe Leriche syndrome (aortoiliac atherosclerotic disease), making it impossible to acccess the femoral artery during a previous coronary angiography attempt. Therefore, the procedure was performed by using the radial artery.
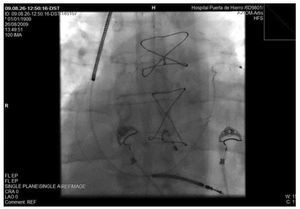
The puncture area was anaesthetized with 2% lydocaine, the radial artery was canalised 1-2 cm proximal to the styloid process of the radius by insertion of a 5 F (Terumo®, Radifocus® Introducer II) radial introducer. After, 2.5 mg of verapamil (antispasmodic drug) and 5000 U of sodium heparin were administered intraarterially. A (Medtronic® Mariner 5F, 4 mm tip) ablation catheter was introduced (Figure 1) retro-aortically until it was positioned over the left His bundle (Figure 2), and ablation was performed without any complications. Times of the procedure, ablation, scopy (30 min, 108 s, 3.05 min, respectively) were not longer than similar procedures performed by the femoral route.

Figure 1. Radial introducer and Medtronic Marinr® 5 F ablation catheter.

Figure 2. Fluoroscopy image that shows the ablation catheter over the His bundle.
At the end of the procedure, the introducer was withdrawn and local manual compression was used, followed by placement of a compressive dressing that was loosened during the following hours without appearance of bleeding or haematoma. The patient was discharged after 24 hours, after confirming normal functioning of the HRT system, with 99.8% stimulation.
Percutaneous radial access is, since in 1989 Campeau4 and in 1993 Kiemeneij et al5 used it for heart catheterization and percutaneous coronary procedures, respectively, an approach ever more frequently used in the cath lab, since it has a lower complication rate, greater comfort for the patient and shorter hospital stay. Its general use is limited by the small size of this artery, which therefore requires the use of smaller calibre catheters with less support, its anatomical variants (such as loops), or arterial spasm, that make catheter advance difficult or impossible, as also the learning curve involved in using this technique as in any other. In the case of electrophysiological studies an added limitation is the simultaneous use of multiple catheters in most of these procedures, which makes it necessary to combine several routes of approach and reduces the advantages of the radial approach.
However, radial access has been shown to be safe, effective, more comfortable for the patient, and has less complications, especially local ones. All these advantages make it a valid alternative to be kept in mind for simple procedures such as, for example, His ablation, or as has recently been published,6 accessory left routes, which can be easily and safely carried out with equal effectiveness using a single catheter.