To study the prognostic impact of preoperative nutritional status, as assessed through the nutritional risk index (NRI), on postoperative outcomes after heart transplantation (HT).
MethodsWe conducted a retrospective, single-center study of 574 patients who underwent HT from 1991 to 2014. Preoperative NRI was calculated as 1.519 × serum albumin (g/L) + 41.7 × (body weight [kg] / ideal body weight [kg]). The association between preoperative NRI and postoperative outcomes was analyzed by means of multivariable logistic regression and multivariable Cox regression.
ResultsMean NRI before HT was 100.9 ± 9.9. According to this parameter, the prevalence of severe nutritional risk (NRI < 83.5), moderate nutritional risk (83.5 ≤ NRI < 97.5), and mild nutritional risk (97.5 ≤ NRI < 100) was 5%, 22%, and 10%, respectively. One year post-transplant mortality rates in these 4 categories were 18.2%, 25.3%, 7.9% and 10.2% (P < .001), respectively. The NRI was independently associated with a lower risk of postoperative infection (adjusted OR, 0.97; 95%CI, 0.95-1.00; P = .027) and prolonged postoperative ventilator support (adjusted OR, 0.96; 95%CI, 0.94-0.98; P = .001). Patients at moderate or severe nutritional risk had significantly higher 1-year post-HT mortality (adjusted HR, 1.55; 95%CI, 1.22-1.97; P < .001).
ConclusionsMalnourished patients have a higher risk of postoperative complications and mortality after HT. Preoperative NRI determination may help to identify HT candidates who might benefit from nutritional intervention.
Keywords
Malnutrition is a common comorbidity in patients with heart failure (HF) and is associated with a poor prognosis.1 Two classic markers of malnutrition (low body mass index2 and hypoalbuminaemia3) are correlated with increased mortality in this patient population. However, neither of these 2 parameters on its own is a reliable indicator of the nutritional status of patients with HF, as either one can be significantly altered as a consequence of the disease. Serum albumin concentration can be affected by conditions inherent to HF, such as chronic inflammation, fluid overload, hepatic congestion, and renal losses,3 while blood volume changes can significantly affect body mass index.4 Therefore, nutritional assessment of patients with HF requires alternative clinical tools that are not subject to such variability.
The nutritional risk index (NRI) is a nutritional evaluation score that has become popular in recent years, thanks to its simplicity and strong prognostic value in different medical and surgical patient populations. Buzby et al.5 originally defined NRI using the formula 1.519 × serum albumin (g/L) + 41.7 × (current body weight [kg] / usual body weight [kg]). It was later suggested to replace the term usual body weight with ideal body weight,6 to avoid the difficulty involved in estimating the usual body weight of some individuals, such as the elderly or those with an unstable fluid balance. The ideal body weight, in contrast, can be easily calculated using simple anthropometric equations. In both the original definition and the modified formula, NRI has been validated as an independent predictor of mortality and adverse clinical events in a wide range of patients with HF, both chronic7,8 and acute,9,10 with reduced7 or preserved8 ejection fraction, as well as in those with advanced disease.10
Malnourished patients undergoing cardiac surgical procedures are at increased risk of postoperative complications.11 In heart transplant (HT) recipients, as is the case in the general HF patient population, low body weight12 and hypoalbuminaemia13 are associated with increased mortality risk. However, until now, the potential usefulness of other markers of nutritional risk in this specific clinical context has not been established.
We sought to analyze the prognostic value of preoperative NRI in patients with advanced HF receiving a HT.
METHODSPatientsThis was a retrospective cohort study of patients older than 18 years who had received an orthotopic HT in our center from April 1991, when the program started, until December 2014. The study data were taken from a local database and supplemented with review of clinical records. The A Coruña-Ferrol Clinical Research Ethics Committee approved the study (Consellería de Sanidade, Xunta de Galicia).
The analysis included only patients for whom the pretransplant NRI could be calculated. This parameter was determined using the modified formula where NRI = 1.519 × serum albumin (g/L) + 41.7 × (actual body weight [kg] / ideal body weight [kg]). Ideal body weight was calculated using the Lorenz formulae, ie height (cm) – 100 – ([height (cm) – 150] / 4) for men and height (cm) – 100 – ([height (cm) – 150] / 2.5) for women. As in previous publications,7,9 when the value of (actual body weight [kg] / ideal body weight [kg]) was ≥ 1, NRI was set at 1. The serum albumin levels and actual body weight used for the preoperative NRI calculation were the closest available to the date of HT in each patient's medical records.
The study patients were classified into 4 nutritional risk categories according to their preoperative NRI, as defined in previous studies7,9: severe nutritional risk (NRI < 83.5), moderate nutritional risk (83.5 ≤ NRI < 97.5), mild nutritional risk (95.7 ≤ NRI < 100) and no nutritional risk (NRI ≥ 100). We compared the baseline clinical characteristics, incidence of adverse clinical events, and post-HT survival of these 4 patient categories.
Postoperative Clinical EventsPrimary graft dysfunction was defined as isolated right ventricular failure or moderate or severe left ventricular failure of the cardiac graft during the first 24hours post-HT, in line with the consensus criteria of the International Society for Heart and Lung Transplantation.14 Cardiac surgical reintervention was defined as any cardiac surgical intervention requiring a repeat sternotomy during the post-HT hospital stay. Postoperative infection was defined as any infection proven by a microbiological isolate and requiring intravenous antibiotic treatment during the post-HT hospital stay. Prolonged mechanical ventilation was defined as invasive mechanical ventilatory support lasting longer than 36hours after HT. Acute rejection was defined as any episode of biopsy-proven grade 2R or above acute cellular rejection,15 any episode of biopsy-proven grade 1 or above antibody-mediated rejection with associated cardiac graft dysfunction,16 or any episode of clinically suspected acute rejection not proven on biopsy that was treated with intravenous bolus steroids, anti-thymocyte globulin, or polyclonal gamma globulin during the post-HT hospital stay.
Information was available on the vital status of all patients at 1 year post-HT. All-cause mortality during this period was the primary event in this study.
Statistical AnalysisIn this article, continuous variables are presented as–mean ± standard deviation or median [interquartile range], depending on the normality of their distribution, while categorical variables are presented as percentages. The baseline characteristics of the different NRI categories were compared using the chi-square test for linear trend for categorical variables and ANOVA with a first-order polynomial contrast for continuous variables.
The Cox proportional hazards model was used to identify independent predictors of mortality during the first year post-HT. First, the preoperative variables that showed a statistically significant association with mortality (P < .05) were selected. These variables were included in a backward stepwise analysis (exit criterion, P > .05) such that the remaining variables (among which was NRI) formed the final multivariable model. To control for potential confounders, the statistical effect of preoperative NRI on post-HT mortality was adjusted using a second extended multivariable model. We forced into this model those variables that showed a significantly asymmetrical distribution over the 4 nutritional risk categories (body mass index, bilirubin, mechanical ventilation, inotropic support, and ischemia time) and the demographic variables (age and sex of recipient), as well as the independent predictors of mortality previously identified from the backward stepwise analysis. The final multivariable model was also used to estimate the adjusted hazard ratio (aHR) for mortality during the first year post-HT for recipients with moderate or severe nutritional risk (NRI < 97.5) compared with recipients with mild or absent nutritional risk (NRI ≥ 97.5).
Using a method similar to that described for the mortality analysis, we employed multivariable logistic regression to identify the predictors of postoperative adverse events for which the univariable analysis showed a statistically significant association (P < .05) with the preoperative NRI values (postoperative infection and prolonged mechanical ventilatory support). Although the univariable analysis also showed a statistically significant association between preoperative NRI and incidence of postoperative stroke, we decided not to perform a multivariable analysis due to the low number of strokes recorded in the study population.
Lastly, the Kaplan-Meier method was used to construct survival curves for the first year post-HT for patients with moderate or severe nutritional risk (NRI < 97.5) and patients with mild or absent nutritional risk (NRI ≥ 97.5). The 2 survival curves were compared using the log-rank test. For all comparisons, a P-value < .05 was considered statistically significant. The statistical analysis was performed with SPSS 20.0.
RESULTSPretransplant Nutritional RiskFrom April 1991 to December 2014, 633 patients > 18 years old received an orthotopic HT in our center. The preoperative NRI could not be calculated in 89 (13%) of them, because information on the pretransplant albumin levels was unavailable. Therefore, the sample analyzed consisted of 574 patients.
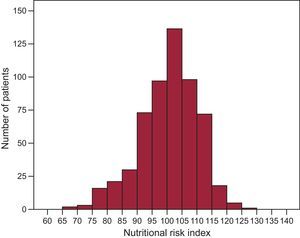
Figure 1 shows the preoperative NRI distribution in the study population. Prior to HT, 33 patients (5%) were at severe nutritional risk (NRI < 83.5); 146 (22%) were at moderate nutritional risk (83.5 ≤ NRI < 97.5), and 63 (10%) were at mild nutritional risk (97.5 ≤ NRI < 100). The mean preoperative NRI was 100.9 ± 9.9.

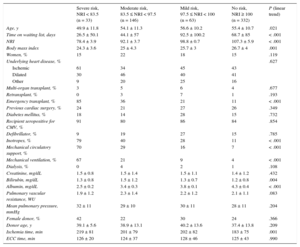
Table 1 shows the baseline clinical characteristics of the study patients by the 4 nutritional risk categories described above. Life support measures, such as inotropes, mechanical ventilation, and mechanical circulatory support were used more frequently before HT in patients with a lower preoperative NRI and in cases of emergency HT (P < .001 for all linear contrasts of these variables). Patients with lower preoperative NRI were also younger (P = .021) and had shorter waiting list times (P < .001), lower body mass index (P = .001), lower serum albumin levels (P = .004) and longer organ ischemia times (P = .001).
Clinical Characteristics of the Study Patients, by Pre-transplant Nutritional Risk
| Severe risk, NRI < 83.5 (n = 33) | Moderate risk, 83.5 ≤ NRI < 97.5 (n = 146) | Mild risk, 97.5 ≤ NRI < 100 (n = 63) | No risk, NRI ≥ 100 (n = 332) | P (linear trend) | |
|---|---|---|---|---|---|
| Age, y | 49.9 ± 11.8 | 54.1 ± 11.3 | 56.6 ± 10.2 | 55.4 ± 10.7 | .021 |
| Time on waiting list, days | 26.5 ± 50.1 | 44.1 ± 57 | 92.5 ± 100.2 | 68.7 ± 85 | < .001 |
| NRI | 78.4 ± 3.9 | 92.1 ± 3.7 | 98.8 ± 0.7 | 107.3 ± 5.9 | < .001 |
| Body mass index | 24.3 ± 3.6 | 25 ± 4.3 | 25.7 ± 3 | 26.7 ± 4 | .001 |
| Women, % | 15 | 22 | 18 | 15 | .119 |
| Underlying heart disease, % | .627 | ||||
| Ischemic | 61 | 34 | 45 | 43 | |
| Dilated | 30 | 46 | 40 | 41 | |
| Other | 9 | 20 | 25 | 16 | |
| Multi-organ transplant, % | 3 | 5 | 6 | 4 | .677 |
| Retransplant, % | 0 | 3 | 7 | 1 | .193 |
| Emergency transplant, % | 85 | 36 | 21 | 11 | < .001 |
| Previous cardiac surgery, % | 24 | 21 | 27 | 26 | .349 |
| Diabetes mellitus, % | 18 | 14 | 28 | 15 | .732 |
| Recipient seropositive for CMV, % | 91 | 80 | 86 | 84 | .854 |
| Defibrillator, % | 9 | 19 | 27 | 15 | .785 |
| Inotropes, % | 79 | 40 | 28 | 11 | < .001 |
| Mechanical circulatory support, % | 70 | 29 | 16 | 7 | < .001 |
| Mechanical ventilation, % | 67 | 21 | 9 | 4 | < .001 |
| Dialysis, % | 0 | 4 | 2 | 1 | .108 |
| Creatinine, mg/dL | 1.5 ± 0.8 | 1.5 ± 1.4 | 1.5 ± 1.1 | 1.4 ± 1.2 | .432 |
| Bilirubin, mg/dL | 1.3 ± 0.8 | 1.5 ± 1.2 | 1.3 ± 0.7 | 1.2 ± 0.8 | .004 |
| Albumin, mg/dL | 2.5 ± 0.2 | 3.4 ± 0.3 | 3.8 ± 0.1 | 4.3 ± 0.4 | < .001 |
| Pulmonary vascular resistance, WU | 1.9 ± 1.2 | 2.3 ± 1.4 | 2.2 ± 1.2 | 2.1 ± 1.1 | .083 |
| Mean pulmonary pressure, mmHg | 32 ± 11 | 29 ± 10 | 30 ± 11 | 28 ± 11 | .204 |
| Female donor, % | 42 | 22 | 30 | 24 | .366 |
| Donor age, y | 39.1 ± 5.6 | 38.9 ± 13.1 | 40.2 ± 13.6 | 37.4 ± 13.8 | .209 |
| Ischemia time, min | 219 ± 81 | 201 ± 79 | 202 ± 82 | 183 ± 75 | .001 |
| ECC time, min | 126 ± 20 | 124 ± 37 | 128 ± 46 | 125 ± 43 | .990 |
CMV, cytomegalovirus; ECC, extracorporeal circulation; NRI, nutritional risk index.
Unless otherwise indicated, all values are expressed as mean ± standard deviation.
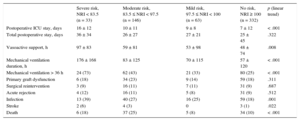
Table 2 summarizes the adverse clinical events that occurred during the in-hospital post-transplant period in the 4 patient subgroups defined by pretransplant NRI. Pretransplant NRI values had an inverse correlation with duration of postoperative vasoactive drug support (P = .008), mechanical ventilation (P < .001), and postoperative intensive care unit stay (P < .001). Total postoperative hospital stay did not have a statistically significant association with preoperative NRI (P = .332).
Clinical Events in the In-hospital Post-transplant Period by Pretransplant Nutritional Risk Index
| Severe risk, NRI < 83.5 (n = 33) | Moderate risk, 83.5 ≤ NRI < 97.5 (n = 146) | Mild risk, 97.5 ≤ NRI < 100 (n = 63) | No risk, NRI ≥ 100 (n = 332) | p (linear trend) | |
|---|---|---|---|---|---|
| Postoperative ICU stay, days | 16 ± 12 | 10 ± 11 | 9 ± 8 | 7 ± 12 | < .001 |
| Total postoperative stay, days | 36 ± 34 | 26 ± 27 | 27 ± 21 | 25 ± 45 | .322 |
| Vasoactive support, h | 97 ± 83 | 59 ± 81 | 53 ± 98 | 48 ± 74 | .008 |
| Mechanical ventilation duration, h | 176 ± 168 | 83 ± 125 | 70 ± 115 | 57 ± 120 | < .001 |
| Mechanical ventilation > 36 h | 24 (73) | 62 (43) | 21 (33) | 80 (25) | < .001 |
| Primary graft dysfunction | 6 (18) | 34 (23) | 9 (14) | 59 (18) | .311 |
| Surgical reintervention | 3 (9) | 16 (11) | 7 (11) | 31 (9) | .687 |
| Acute rejection | 4 (12) | 16 (11) | 5 (8) | 31 (9) | .512 |
| Infection | 13 (39) | 40 (27) | 16 (25) | 59 (18) | .001 |
| Stroke | 2 (6) | 4 (3) | 0 | 3 (1) | .022 |
| Death | 6 (18) | 37 (25) | 5 (8) | 34 (10) | < .001 |
ICU, intensive care unit; NRI, nutritional risk index.
Values are expressed as No. (%) or mean ± standard deviation.
Univariable linear trend analysis revealed a statistically significant increased cumulative incidence in patients with lower preoperative NRI values of postoperative stroke (NRI < 83.5, 6.1%; 83.5 ≤ NRI < 97.5, 2.7%; 97.5 ≤ NRI < 100, 0%; NRI ≥ 100, 0.9%; P = .022), prolonged mechanical ventilatory support (NRI < 83.5, 72.7%; 83.5 ≤ NRI < 97.5, 43.1%; 97.5 ≤ NRI < 100, 33.1%; NRI ≥ 100, 24.5%; P < .001), and postoperative infection (NRI < 83.5, 39.4%; 83.5 ≤ NRI < 97.5, 27.4%; 97.5 ≤ NRI < 100, 25.4%; NRI ≥ 100, 17.8%; P = .022). However, no statistically significant association was observed between preoperative NRI and the cumulative risk of other adverse events, such as primary graft dysfunction, cardiac surgical reintervention, or acute rejection during the post-HT hospital stay.
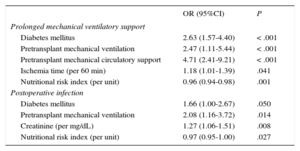
Multivariable logistic regression analysis identified preoperative NRI as a statistically significant independent predictor of prolonged need for postoperative mechanical ventilatory support (adjusted odds ratio [aOR] per unit = 0.96; 95% confidence interval [95%CI], 0.94-0.98; P = .001) and postoperative infection (aOR per unit = 0.97; 95%CI, 0.95-1.00; P = .027), as shown in Table 3. The statistical association between NRI and prolonged mechanical ventilatory support (aOR per unit = 0.96; 95%CI, 0.93-0.98; P < .001) and postoperative infection (aOR per unit = 0.98; 95%CI, 0.95-1; P = .038) did not change substantially when the demographic variables (age and sex) and other clinical variables with asymmetrical distribution in the 4 nutritional risk categories (body mass index, bilirubin, mechanical ventilation, mechanical circulatory support, inotropes, and ischemia time) were forced into the regression model.
Independent Predictors of Prolonged Need for Ventilatory Support and Postoperative Infection Following Heart Transplant: Multivariable Analysis
| OR (95%CI) | P | |
|---|---|---|
| Prolonged mechanical ventilatory support | ||
| Diabetes mellitus | 2.63 (1.57-4.40) | < .001 |
| Pretransplant mechanical ventilation | 2.47 (1.11-5.44) | < .001 |
| Pretransplant mechanical circulatory support | 4.71 (2.41-9.21) | < .001 |
| Ischemia time (per 60 min) | 1.18 (1.01-1.39) | .041 |
| Nutritional risk index (per unit) | 0.96 (0.94-0.98) | .001 |
| Postoperative infection | ||
| Diabetes mellitus | 1.66 (1.00-2.67) | .050 |
| Pretransplant mechanical ventilation | 2.08 (1.16-3.72) | .014 |
| Creatinine (per mg/dL) | 1.27 (1.06-1.51) | .008 |
| Nutritional risk index (per unit) | 0.97 (0.95-1.00) | .027 |
95%CI, 95% confidence interval; OR, odds ratio.
In the first year of follow-up post-HT, 102 patients (17.8%) died. The in-hospital post-HT mortality rates were 18.2%, 25.3%, 7.9%, and 10.2% (P < .001) for recipients with severe, moderate, mild, and absent preoperative nutritional risk, respectively. In the same categories, the overall mortality rates in the first year after HT were 18.2%, 28.8%, 11.1%, and 14.2% (P < .002).
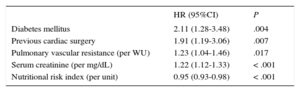
In the Cox multivariable regression analysis, preoperative NRI was identified as an independent predictor of lower risk of death from any cause in the first year post-HT (aHR per unit = 0.95; 95%CI, 0.93-0.98; P < .001) (Table 4). The statistical effect of preoperative NRI on mortality in the first year post-HT did not change substantially with the extended adjustment model that included demographic variables and baseline clinical variables with an asymmetrical distribution over the different nutritional risk groups (aHR per unit = 0.95; 95%CI, 0.93-0.98; P = .001).
Independent Predictors of Mortality in the First Year Post-transplant: Multivariable Analysis
| HR (95%CI) | P | |
|---|---|---|
| Diabetes mellitus | 2.11 (1.28-3.48) | .004 |
| Previous cardiac surgery | 1.91 (1.19-3.06) | .007 |
| Pulmonary vascular resistance (per WU) | 1.23 (1.04-1.46) | .017 |
| Serum creatinine (per mg/dL) | 1.22 (1.12-1.33) | < .001 |
| Nutritional risk index (per unit) | 0.95 (0.93-0.98) | < .001 |
95%CI, 95% confidence interval; HR, hazard ratio.
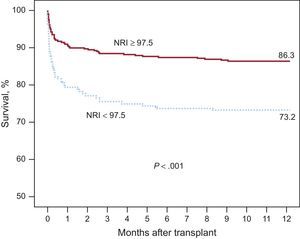
Patients with moderate or severe preoperative nutritional risk, defined as a preoperative NRI < 97.5, had a significantly higher all-cause mortality in the first year post-HT than patients with mild or absent preoperative nutritional risk (aHR = 1.55; 95%CI, 1.22-1.97; P < .001). The Kapan-Meier survival curves for both groups are shown in Figure 2.
DISCUSSION and low or absent preoperative nutritional risk (NRI ≥ 97.5). NRI, nutritional risk index.")
In this cohort of 574 patients who received a HT in the A Coruña University Hospital Complex between 1991 and 2014, a statistically significant independent association was observed between lower preoperative NRI values and lower post-operative survival. Recipients with moderate or severe preoperative nutritional risk, defined as an NRI < 97.5, had a 55% higher risk of death by any cause in the first year post-HT than those with mild or absent nutritional risk. The incidence of postoperative complications such as stroke, prolonged mechanical ventilatory support, and infection was also significantly higher in malnourished patients.
Nutrition is a factor of growing importance in HF physiology. Several previous studies have demonstrated the usefulness of NRI in identifying HF patients at risk of malnutrition-related complications. In the HF population, a correlation has been found between lower NRI values and higher re-admission rates, longer hospital stays, and lower survival.7–10 The strong prognostic value of NRI appears to significantly exceed that of its 2 separate components, is independent of ejection fraction and other comorbidities, and is applicable to both inpatients and outpatients. In the specific setting of refractory HF, NRI can help in the process of selecting candidates for advanced therapies, as it provides increased prognostic value in addition to other validated risk scales.10
More than a third of HT recipients in our series were already at nutritional risk prior to surgery. Using the NRI cutoff points previously defined by other authors,7,9 the percentage of patients with severe, moderate, and mild preoperative nutritional risk was 5%, 22%, and 10%, respectively. This result is similar to those of previous studies, in which the prevalence of nutritional risk ranged from 23% to 48% in different HF patient populations,7–9 although we recognize that NRI is of limited use as an isolated criteria for the diagnosis of malnutrition. In our series, nutritional risk was higher in recipients in more critical clinical situations, such as those requiring inotropic support, mechanical ventilation, or mechanical circulatory assistance while awaiting HT. The association between NRI and mortality remained statistically significant after adjustment for multiple potential confounders, including body mass index. Thus, these results indicate that nutritional status has an independent effect on post-HT prognosis.
Malnourished patients are at higher risk of postoperative adverse events in various surgical situations,17 including major cardiac surgery.18 Malnutrition is a recognized cause of immunodeficiency, increasing the risk of postoperative infection through various pathophysiological mechanisms.19 In critical patients, malnutrition also predisposes to respiratory muscle dysfunction, making early weaning from mechanical ventilation difficult.20 Malnutrition-related complications frequently result in significant increases in postoperative hospital stay, health care costs, and mortality.17,18
Our study has direct implications for clinical practice. First, it confirms the usefulness of NRI as a simple and reliable tool for nutritional assessment in patients with advanced HF. The nutritional status of these patients has considerable prognostic implications and should therefore be closely-monitored, as is done with other risk markers such as functional capacity, hemodynamic status, or target organ function. Given the reduced life-expectancy10 in patients with HF and poor nutritional status, such patients should be assessed early to determine if they may be candidates for advanced therapies such as HT, provided there are no significant comorbidities. Our data also alert us to the lower survival rate after HT in individuals with marked nutritional impairment. Ultimately, serial determination of NRI could help identify HT candidates that could benefit from targeted nutritional interventions while awaiting transplant.21 For some of these patients, implantation of a long-term ventricular assist device could be a reasonable option, given the good outcomes in nutritional improvement that have been demonstrated with this therapy.22
LimitationsOur study has some methodological limitations. Given its retrospective design, it is subject to the potential selection bias and information bias inherent to this type of study. To control any potential confounding bias, rigorous multivariable adjustment was performed. Nonetheless, we cannot entirely rule out that another untested variable could have interfered with the observed statistical associations. The single-center setting of the study meant that the external validity of the results could not be guaranteed, therefore we may not be able to extrapolate our conclusions to other patient populations. The selection of a historic cohort spanning a long time period is in itself a limitation when interpreting the study results, which could have been affected by historic changes and improvements in the perioperative treatment protocol for HT patients.
The lack of information on preoperative albumin levels led to the exclusion of 89 HT recipients from the study, but it seems unlikely that the inclusion of these patients in the analysis would have led to a significant change in the observed results. Lastly, as we retrospectively used previously-collected data, it is highly likely that the time elapsed from the preoperative determination of albumin level and body weight to HT varied between study patients.
CONCLUSIONSOur study confirms the clinical usefulness of NRI as a screening tool for the nutritional status of patients with advanced HF who are candidates for HT. Malnourished recipients had a significantly higher incidence of post-HT complications such as infection, late weaning from invasive mechanical ventilation, and stroke, as well as longer postoperative intensive care stay, and lower survival. These results indicate the need for future studies to assess the potential clinical benefit of targeted interventions to improve the nutritional status of HT candidates.
FUNDINGSeveral authors belong to the A Coruña Biomedical Research Institute Advanced Heart Failure and Heart Transplantation Research Group. This group regularly receives funding for the conduct of its scientific activities from the Instituto de Salud Carlos III (Carlos III Institute of Health) Cardiovascular Research Network, Ministry of Economics and Competitiveness, Government of Spain.
CONFLICTS OF INTERESTNone declared.
- –
Malnutrition is a common comorbidity in patients with HF and is associated with increased mortality.
- –
The NRI, a score calculated from serum albumin levels and the ratio of the patient's actual weight to usual weight (or, if unavailable, the ideal weight), has been validated as a strong prognostic predictor in this population.
- –
The NRI may have a similar role in HT recipient patients, but so far this specific group has not been studied.
- –
The study confirms the effect of preoperative nutritional status on HT outcomes and supports the usefulness of NRI as a prognostic marker in this specific clinical context.
- –
The findings indicate that the serial determination of NRI could help identify HT candidates that could benefit from targeted nutritional interventions while awaiting transplant.
The authors would like to thank Zulaika Grille-Cancela, Paula Blanco-Canosa, Cristina Costa-Graña, and Carmen Naya-Leira for their contribution to this study.