Keywords
INTRODUCTION
Anemia is frequent in patients with heart failure (HF) and prevalence is in the 5%-55% range depending on the criteria used and population studied.1 Degree of anemia correlates with seriousness of HF2-6 and prognosis.4-10 Anemia in patients with HF is probably multifactorial and may be due to reduced intestinal iron absorption,11-14 increased cytokine production of tumor necrosis factor alpha in particular which causes bone marrow depression, renin-angiotensin-aldosterone system activation causing sodium and water retention with dilutional anemia, renal insufficiency that frequently affects patients with HF (partly due to vasoconstriction and renal ischemia) and entails reduced erythropoietin production, loss of erythropoietin and of transferrin due to the coexistence of proteinuria, angiotensin converting enzyme (ACE) inhibitor treatment which, especially at high dosage, can influence erythropoietin production in the kidney and bone marrow response to this, antiplatelet agents or anticoagulants which can contribute to the presence of anemia and cause blood loss. Moreover, anemia itself contributes to HF requiring increased cardiac output to deliver oxygen to the tissues, which produces sympathetic stimulation with vasoconstriction and tachycardia. Renal vasoconstriction activates the renin-angiotensin-aldosterone system with reduced renal flow and water retention leading to secondary kidney failure that worsens anemia and, in the long-term, causes hypertrophy and ventricular remodeling that aggravates HF.
Awareness of the high prevalence of anemia in the population attending our HF Unit15 led us to evaluate the prognostic significance of plasma hemoglobin (Hb) levels in terms of mortality and HF-related admissions at 1 year follow-up.
PATIENTS AND METHODS
In our multidisciplinary HF unit, we prospectively gathered first visit Hb level data on all patients together with other demographic, clinical, biochemical, and therapeutic parameters. We then determined the prevalence of anemia, defined a priori as Hb<12 g/dL, which is considered the lower limit of normal in adult males and post-menopausal women.16 In a cross-sectional study, we correlated Hb levels with various parameters.15 Patients with the criterion of admission for HF as their principal problem were referred to the HF unit from the hospital Cardiology and Internal Medicine services and, to a lesser extent, from Emergency Room, other hospital services and outpatient cardiologists in the area. At l year, we correlated plasma Hb levels with mortality and HF-related admission in 337 patients. We also analyzed mortality and HF-related admission in terms of presence or absence of anemia (Hb<12 mg/dL).
Statistical analysis was performed with SPSS for Windows 11.0. We considered P<.05 statistically significant. Correlations of Hb levels (with a normal distribution) and continuous variables were analyzed by linear regression and associations with dichotomous parameters by the Student t test. In univariate analysis of Hb level association with different parameters, statistical significance was adjusted with Bonferroni correction. Univariate analysis of associations between Hb levels and mortality or HF-related admission was by the Student t test. Subsequently, to adjust Hb levels for clinical parameters, we performed multivariate logistic regression analysis using the forward stepwise method and including 1-year mortality and HF-related admission as dependent variables in addition to the independent variables listed in Table 1. We also used logistic regression analysis to calculate the odds ratio (OR) of the variable anemia.

The study was carried out fulfilling the personal data protection law and in agreement with the international recommendations for clinical research of the World Medical Association Declaration of Helsinki.
RESULTS
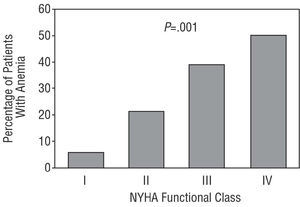
Between August 2001 and March 2003, 341 patients were admitted to the HF unit. Survival status and incidence of HF-related admission at 1 year follow-up are known for 337 of these patients (72% men; mean age, 65.4±10 years). Demographic characteristics appear in Table 2. Table 3 shows correlations between Hb level and various parameters with initial statistical significance and statistical significance adjusted with Bonferroni correction. Given our definition of anemia, this was present in 30% of patients. The relationship between prevalence of anemia and NYHA (New York Heart Association) functional class is clear (Figure 1).



Figure 1. Percentage distribution of patients with anemia by functional class for heart failure (NYHA).
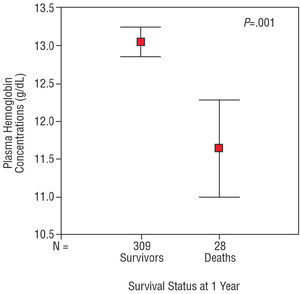
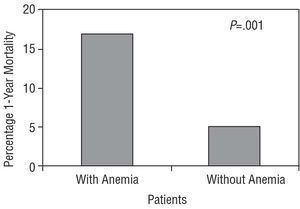
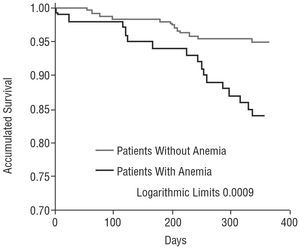
During the first year of follow-up, 28 (8%) of the 337 patients died and 158 HF-related hospitalizations were recorded in 66 patients (Table 4). Hemoglobin levels correlated significantly with 1-year mortality (patients who were alive 13±1.7 g/dL, patients who died 11.6±1.7 g/dL; P<.001) (Figure 2). We also found significant correlations with HF-related admission (patients without admissions 13.1±1.7 g/dL, patients with ≥1 admissions 12.2±1.7 g/dL; P<.001). In the logistic regression analysis, Hb levels remained in the model and maintained statistical significance in terms of 1-year mortality (OR=0.60; 95% CI, 0.46-0.79; P<.001) and HF-related admission (OR=0.79; 95% CI, 0.66-0.95; P=.013). Given our definition of anemia as Hb<12 g/dL, anemia was present in 30% of patients. One-year mortality was 17% in patients with anemia and 5% in those without (P<.001) (Figure 3). Risk of death during the first year of follow-up was ≥3 times greater in patients with anemia (OR=3.5; 95% CI, 1.62-7.86; P=.002). Figure 4 shows Kaplan-Meier survival curves for patients with and without anemia. Some 31% of patients with anemia had ≥1 HF-related hospitalization versus 15% of patients without anemia (P=.001). Risk of HF-admission during the first year of follow-up was ≥2 times greater in patients with anemia (OR=2.3; 95% CI, 1.37-4.17; P=.002).


Figure 2. Graph showing means and standard deviations of hemoglobin levels for survivors and patients who died at 1 year of follow-up.

Figure 3. One-year mortality in patients with and without anemia on initial visit.

Figure 4. Kaplan-Meier survival curves for patients with and without anemia.
DISCUSSION
Anemia is present in 5%-55% of patients with HF depending on selection criteria and on the definition of anemia used.1 In our series, which corresponds to the general population attended in a multidisciplinary HF Unit of a tertiary hospital without a transplant program, prevalence of anemia (defined as Hb<12 g/dL) is approximately in the center of this range. Anemia in HF is multifactorial. One of the most widely published series (12 065 patients) reported 58% of patients presented anemia of chronic disease.4 In a much smaller series (37 patients) that analyzed data on hemodilution, this was the cause of anemia in 46% of patients.6 Our series did not include data on hemodilution. One highly significant aspect of our population is the clear relationship between presence of anemia and NYHA functional class. This relationship is described by other authors2,5,6 although in some series3 Hb levels vary little when comparing functional classes and significant differences are found only by comparing classes I and II with classes III and IV. The relationship between Hb levels and HF-related admissions in the previous year is also highly significant, a phenomenon also observed by Felker et al.9 Another significant finding is the relationship seen in our population between lower Hb levels and the coexistence of diabetes, a phenomenon observed by some authors9 but not by others.3,5 Ezekowitz et al,4 reporting a series including 12 065 patients, found a relationship between diabetes and anemia of chronic disease but not between diabetes and all anemia. In any case, our multivariate analysis showed the relationship between diabetes and Hb levels lost statistical significance. We were also surprised to see the relationship between plasma Hb levels and cholesterol (higher cholesterol levels associated with higher Hb levels). Horwich et al5 also found similar data. The malnutrition that accompanies advanced HF may play a role in this relationship but we do not have sufficient data to support this theory. Although Horwich et al5 discuss the possible relationship between anemia and malnutrition, they do so on the basis of the relationship observed with albumin levels and body mass index, without reference to cholesterol5.
More and more attention is being paid to anemia in patients with HF due to the relationship between anemia and HF prognosis which, in spite of all the new HF drug treatments available, continues to be poor.17 Our data confirm that in Spain, anemia is clearly associated with a poor prognosis of HF. This association was reported by other authors4-9 for mortality and HF-related need for readmission. Moreover, the same association was found in hospitalized patients4,7,9 and out-patients.5,8 Nonetheless, we found that plasma Hb levels maintained statistical significance in the multivariate analysis for mortality and HF-related admission. Anemia is reported to be an independent prognostic factor in patients with HF in more extensive series.5,7-9 Mozaffarian et al8 found a 1% reduction in hematocrit was associated with a 3% increase in risk of death in a series of 1130 patients with a mean follow-up of 15 months. Felker et al9 found a 12% increase in the risk of suffering an event per 1 g/dL reduction in plasma Hb decrease in relation to a combined outcome of death and hospitalization at 60 days in a series of 949 patients9. Kosiborod et al7 also found a 2% increase in 1-year mortality per 1% reduction in hematocrit and a 2% increase in risk of readmission at 1 year per 1% reduction in hematocrit. We found a 40% reduction in risk of death at 1 year per 1 g/dL increase in Hb and a 21% reduction in risk of HF-related admission at 1 year. This supports the argument in favor of correcting anemia when treating HF as the use of erythropoietin and iron has been shown to benefit patients2,18,19. On the other hand, in a small series, Androne et al6 found that, in patients with HF, anemia due to hemodilution had a worse prognosis than true anemia, probably because of the greater volume overload and higher pulmonary capillary wedge pressure that hypervolemia generates.
Whether the association between anemia and a worse prognosis in patients with HF is chance or whether anemia is simply a risk marker remains unclear. The initially favorable results of these studies with erythropoietin and iron, the prejudicial hemodynamic effects and the chance that anemia may favor myocardial ischemia support the possible cause-effect relationship. Treatment of anemia in patients with HF has improved prognosis for admissions2,18,19 and significantly improved functional capacity20.
Limitations of the Study
The study sample was drawn from the general population with HF attended in a specific, multidisciplinary HF unit of a tertiary hospital but this does not mean a complete absence of selection within the total population of patients with HF. The patients enrolled were mainly drawn from the Cardiology service, predominantly male, with ischemic etiology and relatively young. Therefore, the results can not necessarily be extrapolated to the overall population with HF. Hemoglobin level data we analyzed were obtained at a specific time (on first visit to the unit) and we did not evaluate changes occurring during the evolution of the illness or to patients' clinical situation. We do not have data on causes or treatment of anemia so these were not analyzed in the present study.
CONCLUSIONS
Hemoglobin levels are important, independent prognostic indicators of mortality and HF-related admissions in patients with HF. The prevalence of anemia is seen to be important in a general population attended in a multidisciplinary HF unit. Hemoglobin levels correlate with a range of demographic, clinical, biochemical and therapeutic parameters, especially, age, gender, functional class and plasma levels of urea and cholesterol.
ACKNOWLEDGEMENT
To Dr. J. López-Ayerbe for his collaboration and help in constructing the HF Unit database and in analyzing the results.
Correspondence: Dr. J. Lupón.
Unitat d'Insuficiència Cardíaca. Hospital Universitari Germans Trias i Pujol.
Ctra. del Canyet, s/n. 08916 Badalona. Barcelona. España.
E-mail: jlupon@ns.hugtip.scs.es