To the Editor:
Although ST-segment elevation in precordial ECG leads is characteristic of anterior left ventricular infarction, it may also be observed in patients with proximal right coronary occlusion.1 We describe a rare case of a patient presenting with ST-segment elevation in precordial leads V1-V3 due to occlusion of the ventricular branch of the right coronary artery during percutaneous coronary angioplasty.
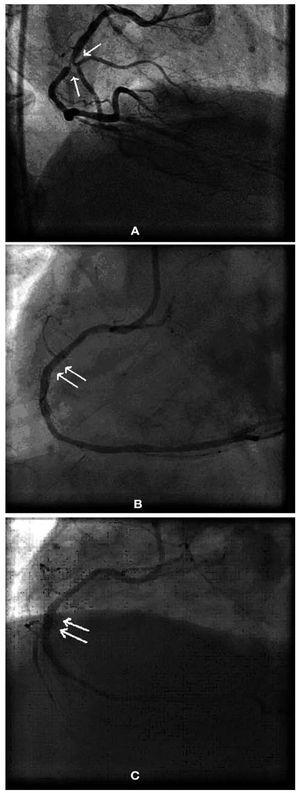
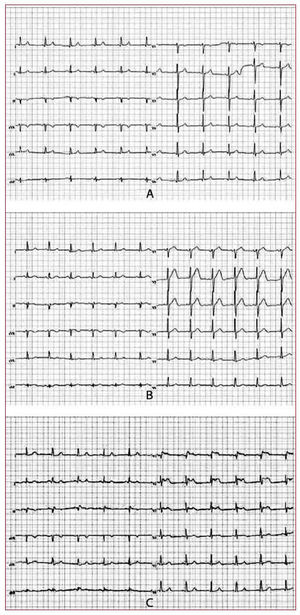
A 69-year-old man was admitted to our department for a follow-up angiogram of a stent that had been successfully implanted in the left main (LM) coronary artery 6 months earlier. The follow-up angiogram revealed excellent results for the LM coronary artery stent (confirmed by intravascular ultrasound catheter) and a significant lesion in right coronary artery (Figure 1A). The results of an electrocardiogram (ECG) were normal (Figure 2A). Direct stenting with a drug-eluting stent was performed with subsequent right ventricular (RV) branch occlusion (Figure 1B). A few minutes after the procedure had been completed, the patient complained of chest pain and the presence of ST elevation in V1-V3 leads was observed on ECG (Figure 2B). The patient immediately underwent a second procedure for a possible complication in left coronary artery but no changes were detected. The RV branch was partially recanalized but was still severely compromised (Figure 1C), while ST elevation in precordial leads was typical for progressive anterior myocardial infarction (Figure 2C). The ECG changes resolved by the next day. Troponine-I and CK-MB (mass) were slightly increased (0.53 and 7.2 µg/L, normal ≤0.13 and ≤3.5 µg/L, respectively) 6 hours later and peak values were recorded the next day (12.44 and 89.5 µg/L, respectively). Isolated occlusion of a right ventricular branch may appear as an acute anterior ischemia that is thought to be a mirror image of right ventricular ischemia.

Figure 1. The arrows indicate, A: a significant lesion in right coronary artery; B: direct stenting with a drug-eluting stent, performed with subsequent right ventricular branch occlusion; and C: the right ventricular branch partially recanalized, but still severely compromised.

Figure 2. The ECG was normal (A), while ST elevation in V1-V3 leads appeared on ECG (B), and ST elevation in precordial leads was typical for progressive anterior myocardial infarction (C).
In our case, and in contrast to other published cases, the patient was asymptomatic, with no previous myocardial infarction or inferior infarction requiring his transfer to the cath lab for primary angioplasty. Right coronary artery stenosis was one finding in the follow-up angiogram for the left main stent. The ECG abnormalities (ST elevation only in precordial leads V1-V3) appeared shortly after right ventricular branch occlusion, with no changes in II, III, aVF or right precordial V2R-V6R leads.
The ECG changes accompanying right ventricle infarction vary widely and depend on the coexisting electrical force ratio between the ischemic right ventricular free wall and the left ventricular inferior wall. Isolated RV myocardial infarction (MI) yields an ST segment elevation in the precordial leads, whereas its combination with inferior left ventricular MI suppresses this ST segment elevation in the precordial leads and yields an ST segment elevation in leads II, III, and aVF.2-4 Massive ST-segment elevation in precordial and inferior leads in RVMI has also been observed but is extremely rare.5 Thus, ST elevation in precordial leads should not exclude an infarction of the right ventricle that demands a treatment different from that of the anterior infarction.
In conclusion, isolated RV branch occlusion may be accompanied by ST-segment elevation in left precordial leads. This should not be assumed to be indicative of anterior MI in patients presenting with acute inferior MI. It is important that physicians and, especially, interventional cardiologists be aware of this entity and protect patients from unnecessary interventions.