To the Editor:
In the July issue of the Revista Española de Cardiología,1 Bayés suggested a change in the terminology used to describe myocardial infarctions. Basing his arguments on a correlation between electrocardiography and magnetic resonance imaging (MRI),2,3 this author rejects the classification put forward by Perloff4 of greater curvature of the inferobasal left ventricular (LV) wall and attributes the posterior infarction pattern to what he calls the lateral wall, in keeping with a consensus document.5
In 1999 a multidisciplinary group6 called for the use of anatomically correct terminology for Wolff-Parkinson-White (WPW) syndrome and other arrhythmias. Using MRI and fluoroscopy, they showed that the lateral mitral annulus has a posterior position, near the spine, which explains why pre-excitation by accessory pathways in this area shifts the QRS vectors forward, with positive
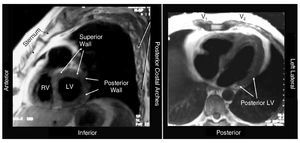
QRS in V1 and V2. Unfortunately, these observations were not taken into consideration by the working group that proposed a dissociated terminology for the anatomical position of the heart in 2002.5 The left anterior oblique MRI views (Figure 1), including those of Bayés et al,1,2 do not perfectly express the anteroposterior or mediolateral position, but do reflect the position with respect to the sternum, demonstrating a posterior position of the "lateral" basal segments next to the spine. Furthermore, computerized navigation reconstruction of the left ventricle allows models of the left ventricle to be created in its true position and shows infarction areas in a posterior position (Figure 2).

Figure 1. Left anterior (left) and transverse (right) oblique views of the heart showing the extremely posterior position of the basal portions of the lateral wall. The superior position of the segments known as "anterior" is also shown.

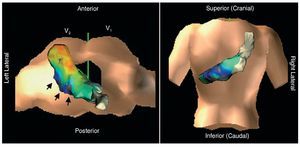
Figure 2. Virtual anatomical reconstruction of the left ventricle (Navx®) superimposed on the torso image, showing the actual anatomical position (not the size). The infarct area (gray, blue, and violet) indicated with arrows has a posterior position.
Another anomaly of the proposed nomenclature1,3,5 is that it fails to recognize a superior wall, which is clearly evident on MRI (Figures 1 and 2). If we were to recognize this location as the site of what is now termed anterior infarctions, we would have a simple explanation of why they are recorded from the top (aVL) and why the ST is paradoxically depressed at the inferior leads.7
The use of topographically correct terminology may be of help to understanding the relationships between the anatomy and the diagnostic patterns in the ECG and other examinations. In another publication,8 we have shown how this facilitates an understanding of normal and abnormal ECGs.
In short, the problem with the ECG is that it remains faithful to the anatomy and tells us that the left ventricle has posterior and superior segments. Our effort to ignore this reality is the actual problem.