To the Editor:
Pleuropericardial cyst is a rare lesion, with a benign clinical course in most cases, that is detected incidentally on chest x-ray and may be confused with a neoformative process of the lung. We present a case of pleuropericardial cyst in a female smoker.
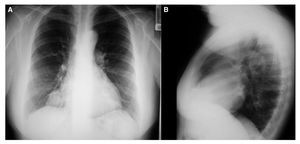
A 55-year-old woman came to the emergency room for chest pain. Relevant history included smoking (15 pack-years) and diabetes treated with oral hypoglycemic agents. She had not presented respiratory or cardiovascular symptoms of interest to date. Because the medical history and the initial physical examination revealed no relevant data, a hemogram and biochemistry were requested, with all results within normal limits. Electrocardiography was normal and abdominal sonography ruled out acute bile disease. The posteroanterior chest x-ray showed a rounded, right paracardiac image of approximately 5 cm (Figure). The image was not seen in a previous x-ray brought by the patient (from 6 years earlier) and therefore, she was admitted by our department for further study of the lesion.

Figure. Posteroanterior (A) and lateral (B) chest x-ray view showing the pleuropericardial cyst in the right costophrenic angle.
The next test requested was a chest computed tomography (CT), which disclosed a lesion measuring 6 cm at its largest diameter adjacent to the right side of the pericardium, with no change observed after administration of intravenous contrast material. The lesion had cystic characteristics and no definable wall, corresponding radiologically to an uncomplicated pleuropericardial cyst; the rest of the study was normal.
The patient was discharged and an outpatient echocardiography was scheduled, which confirmed the diagnosis of uncomplicated pleuropericardial cyst. She remained asymptomatic, and clinical follow-up was carried out by the outpatient clinic, with echocardiograms performed regularly.
The incidence of pleuropericardial cyst has been estimated at 1 per 100 000 cases, accounting for 5%-10% of all mediastinal tumors. Most are congenital, although several acquired cases with an infectious, inflammatory, or traumatic etiology have been described. They are usually identified in the fourth or fifth decade of life.1 The most frequent site is the right costophrenic angle (70%), followed by the left costophrenic angle (10%-40%), although other unusual sites have also been reported, for instance, the vascular hila, the superior mediastinum, or the left heart border.2 There are usually no symptoms, with the cyst being an incidental finding on conventional chest x-ray, identified as a homogeneous, radio-opaque oval lesion. However, episodes of chest pain, tachycardia, persistent cough, and cardiac arrhythmias have been described. These symptoms can result from the pressure of the cyst on adjacent organs. This cyst generally presents a favorable prognosis, although its natural history is not completely known.3 The literature reports cases ranging from spontaneous disappearance to recurrence after surgical resection, as well as serious, even fatal complications such as cardiac tamponade due to rupture, cardiogenic shock, erosion of the vena cava, torsion, cardiac compression, or infection of the cyst.3 The differential diagnosis is extensive and includes, among others, Morgagni hernia, pericardial fat, ventricular aneurysm, cardiac or bronchogenic tumors, and evidently all other masses of the middle mediastinum.2 Authors agree that an asymptomatic onset is a sign of good prognosis and that the additional examinations of choice are chest CT and echocardiography.3 Nevertheless, when there is hemodynamic compromise, transesophageal echocardiography may be indicated to confirm compression of the large vessels or the cardiac cavities by the cyst. Magnetic resonance has also been proposed as a useful imaging technique for this entity. In the event that the cyst is radiologically of inconclusive cystic typing or the attenuation coefficient within the cyst is greater than water, percutaneous puncture is indicated to rule out neoplastic processes or superinfection. Authors recommend conservative treatment and follow-up with chest CT or echocardiography in the asymptomatic cases. Surgical treatment is reserved for the following situations: presence of symptoms, large cysts, atypical sites, or near large vessels.4 Cyst puncture is the treatment of choice according to most current protocols,5 although videoendoscopic surgical techniques are increasingly becoming the therapeutic modality preferred by chest surgeons. Nevertheless, definitive resection by thoracotomy is indicated in complicated cases or when the cyst is adhered to surrounding structures.
In the case described above, the patient is asymptomatic from the cardiopulmonary point of view, and the pleuropericardial cyst was found incidentally in a routine chest x-ray to study the abdominal pain that led to consultation in the emergency department, with subsequent confirmation by echocardiographic study. Therefore, although pleuropericardial cyst is a rare lesion, it should be considered in the differential diagnosis of mediastinal masses.