Keywords
INTRODUCTION
Recently contrast-enhanced MSCT coronary angiography has emerged as a powerful non-invasive diagnostic modality to visualize the coronary arteries and to detect significant coronary stenoses.
The sometimes striking images, in particular the three-dimensional volume rendered images of the heart and coronary arteries, are so powerful and convincing and provide a strong incentive for cardiologists and radiologists alike to purchase the newest 64 CT-scanner--the newest "must-have" equipment. This is further stimulated by the commercial advertisements of CT-scanners by involved vendors which are highly suggestive and persuasive to obtain a CT-scanner for direct use in daily clinical practice. And although the real place of CT-coronary angiography in clinical cardiology still has to be determined, the potential of CT-scanners has sparked off an intense debate between cardiologists and radiologists about the leadership role (and attendant reimbursement) of CT cardiac imaging. In this article we review the published data, and put the often overheated expectations in the right perspective.
Current Status of MSCT Coronary Angiography: 4 to 16-Slice CT Scanners
The initial reports about 4-slice CT-scanners, demonstrated promising results to non-invasively detect significant coronary stenoses.1-10 The technique was too limited to reliably detect coronary stenoses because: 1) the acquisition time and thus the breathhold was too long (30 to 40 seconds) causing respiratory motion artefacts; 2) the temporal resolution was too long (500 ms tube rotation speed with resultant temporal resolution of 250 mseconds) causing cardiac motion artefacts; and finally 3) the limited spatial resolution in particular in the Z-axis, all of which resulted in the fact that approximately 20% to 30% of the eligible coronary segments were non-evaluable.
The 16-slice MSCT scanner has significantly improved in terms of temporal resolution (210 ms) and spatial resolution (in-plane resolution approximately 0.4*0.4 mm and minimum section thickness of 0.75 mm) while the new tube design, allowing higher output, offered a better signal to noise ratio. Comparative invasive angiographic studies have shown that the diagnostic performance of 16 slice MSCT coronary angiography to detect significant coronary stenosis is high with sensitivities ranging from 63% to 98% and specificities from 95% to 98% (Table 1).11-20 Pooling the results of these studies reveals an average sensitivity of 87% and a specificity of 96%. This is achieved in roughly 90% of all coronary segments while 10% of the coronary segments were not able to be analysed due to motion-artifacts or severe calcification. These limitations render the 16-slice CT-technique unreliable for routine clinical use and it is of note that the reported sensitivities and specificities were obtained in the larger proximal, mid and distal coronary segments that had lumen diameters more than 1.5 to 2 mm.

64-Slice CT Scanner: the Newest Generation
Significant technical advances in CT-technology have been introduced with an almost unprecedented speed during the recent few years, which has culminated in the production of a 64-slice CT scanner which currently is available for clinical testing and offered by the various vendors (Siemens, Philips, General Electric, and Toshiba). The 64-CT scanners from the various vendors differ slightly in design and configuration but all scanners feature a high temporal and spatial resolution and fast coverage of the entire heart with an acquisition time ranging from as low as 6 seconds to as high as 12 seconds.
In our department we have evaluated the diagnostic performance of the 64-slice CT scanner (Siemens, Forchheim, Germany) (Figures 1 and 2). We investigated 51 patients (predominantly males) with an average age of 61 years. We included the clinically relevant segments of the entire coronary tree and excluded only the smaller segments less than 1 mm in diameter (very distal branches and side branches) from analysis.21 We found a sensitivity of 95% and specificity of 97% to detect a significant coronary stenosis when compared with invasive diagnostic coronary angiography.

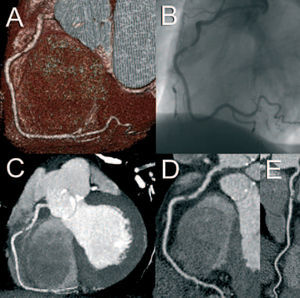
Figure 1. Volume-rendered (A), maximum intensity projected (C) and 2 orthogonal curved multiplanar reconstructed CT images (D, E) depicting a focal non-calcified significant lesion in the proximal right coronary artery, which was confirmed on the conventional angiogram (B).

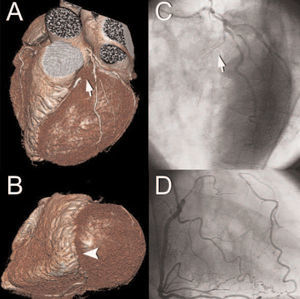
Figure 2. Volume-rendered MSCT images (A, B) providing a 3-dimensional overview of the left coronary artery and revealing a chronically occluded left anterior descending coronary artery (LAD, arrow) with collateral filling (arrowhead) from the posterior descending coronary artery (PDA), which was confirmed on conventional angiogram.

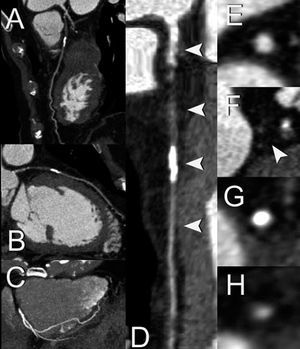
Figure 3. Curved orthogonal multiplanar reconstructed CT images (A, B) showing the occluded trajectory of the LAD. A maximum intensity projected CT image (C) suggests the presence of a collateral artery originating from the PDA throughout the apex towards the distal LAD, which clarifies the luminal enhancement distal of the chronic total occlusion (CTO). After creating a 3-dimensional central lumen line using dedicated software (Vesselview®, Siemens, Forchheim, Germany), the LAD can be displayed throughout its course (D) in a single image, after which cross-sectional images orthogonal to the lumen can be obtained. These cross-sectional images show before and distal to the occlusion a contrast-enhanced patent lumen (E, H), whereas non-calcified (F) and calcified plaque tissue (G) is visualized at the level of the CTO.
Leschka et al reported their experience with the 64 CT-scanner in the evaluation of 67 symptomatic patients with an average age of 60 years22. The sensitivity was 94% and the specificity was 97% to detect a significant coronary stenosis. None of the coronary segments needed to be excluded from analysis although only coronary segments larger than 1.5 mm were included.
Limitations of MSCT Coronary Angiography
Despite significant technological progress and increasing experience with the evaluation of MSCT coronary angiography a number of shortcomings remain (Table 2). CT coronary angiography cannot be used in patients with persistent irregular heart rhythm (atrial fibrillation) or frequent extrasystoles which preclude reconstruction of coronary images. Severe calcification poses 2 problems: 1) it obscures the underlying lumen and thus detection of a significant stenosis, and 2) due to its blooming effects the severity of an adjacent stenosis may be overestimated.

Fast heart rates (>70 beats per minute) are associated with cardiac motion-artifacts or unsharp images because the end-diastolic reconstruction time required for motion-free coronary reconstruction imaging is reduced.23 Reduction of the heart rate with oral or intravenous β-blockade remedies this problem in the majority of the cases. The temporal resolution can be further reduced by use of bisegmental or multisegmental reconstruction algorithms that combine data from 2 or more cardiac cycles and thus prevent the occurrence of cardiac motion blurred images. However, these algorithms are most optimal when the heart rate is constant, the ECG signal is reliable and no arrhythmia occurs, since they rely on an identical cardiac contraction pattern with time-consistent positioning of the cardiac structures during each consecutive heart cycle. The radiation exposure associated with CT-scanning is of major concern. Morin et al estimated the effective radiation-dose of 4-slice MSCT coronary angiography to be between 9.3 and 11.3 mSv.24 Hunold et al used a phantom to measure the radiation-dose and reported this to be 6.7-10.9 mSv for men and 8.1-13.0 mSv for women.25 Phantom experiments with the 16-slice MSCT resulted in a radiation-dose of 8.1 mSv for men and 10.9 mSv for women.26 Reduction of the radiation-dose can be achieved by utilization of the tube modulation mode during scanning. By lowering the x-ray tube output during scanning in systole (usually these data are not used for coronary image reconstruction) and using the nominal output during diastole (data used for image reconstruction) one can reduce the effective radiation-dose by nearly 50%.27 However by using the tube modulation mode, one relies heavily on the presence of a similar R-R interval during scanning which is a prerequisite to reconstruct the coronary images during the same end-diastolic period. Another drawback of the use of the tube modulation mode is the lack of systolic data, which in our experience are useful in about 20% of the cases to reconstruct blur free images. Lastly, image resolution due to x-ray attenuation may be compromised in obese patients who represent an increasing portion of the population.
CT Coronary Angiography: Current Status
Contrast-enhanced CT- coronary angiography, including the 64-slice CT-technology, should be considered as a research tool. The reported data about CT-coronary angiography are increasingly more promising showing that the detection or exclusion of a significant coronary stenosis becomes more reliable suggesting that the technique is applicable in the clinical situation. However, presented data should be viewed with sound scepticism before we can fully embrace this non-invasive technique as a clinically reliable alternative to invasive diagnostic coronary angiography. The CT-technique fails in case of persistent arrhythmia, frequent extrasystoles and severe calcification and this occurs quite frequently alone or in combination in the elderly population (>70 years) where the incidence of symptomatic coronary artery disease is most frequent. Furthermore, a new technique is only useful as an alternative diagnostic technique if it is reliable for all relevant coronary segments without exclusion of non-diagnostic segments. Currently CT-coronary angiography may be a viable alternative to invasive coronary angiography to: 1) exclude significant coronary obstructions in patients with atypical chest pain; 2) to establish the abnormal course of coronary anomalies; and 3) perhaps be reliable enough to refer symptomatic patients to percutaneous coronary intervention on the basis of the CT-findings in a selected population with a slow, stable heart rate and no or mild calcification.
Further studies are desperately needed to establish the clinical role of CT-coronary angiography, using 64-slice CT-scanners or the next generation CT-scanners, in a wide spectrum ranging from asymptomatic individuals to atypical and typical stable angina to patients presenting with acute coronary syndromes. However, we firmly believe that CT-coronary angiography is a powerful non-invasive technique, that in the near future will mature into a clinically applicable non-invasive coronary imaging technique. The presence of a non-invasive coronary imaging technique will significantly improve our understanding and management of coronary artery disease.
Correspondence: Dr. P.J. de Feyter.
University Hospital Rotterdam. Department of Radiology and Cardiology.
Thoraxcenter Ba 591.
P.O. Box 2040. 3000 CA Rotterdam. The Netherlands.
E-mail: p.j.defeyter@erasmusmc.nl