To the Editor,
We present the case of an 82-year-old woman with severe aortic stenosis who was admitted to the hospital due to heart failure with New York Heart Association class III. Given the high surgical risk (EuroSCORE, 24%) and the associated comorbidity, surgical replacement was ruled out and the decision was made to perform transcatheter aortic prosthesis implantation.
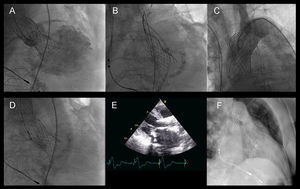
The procedure was carried out by femoral approach and involved the implantation of a 26-mm CoreValve prosthesis according to the standard technique.1 Moderate-to-severe aortic insufficiency was observed due to the low implantation of the prosthesis (Figure 1A), and the attempt was made to relocate it by traction using a snare catheter (Figure 1B).

Figure 1. A: angiographic image showing moderate-to severe aortic insufficiency due to low implantation of the prosthesis. B: traction using a snare catheter. C: relocation of the prosthesis in ascending aorta; the patency of the supraaortic vessels can be observed. D: implantation of the second prosthesis. E: echocardiographic follow-up showing the situation of both prostheses. F: computed tomographic image showing the situation of both prostheses.
After a few minutes of continuous traction, the prosthesis migrated toward the ascending aorta, where it remained fixed. Several angiographic images were obtained, and we confirmed that the prosthesis did not move and that the supraaortic vessels were patent (Figure 1C).
A second prosthesis was implanted with no complications (Figure 1D), the gradient disappeared and the residual aortic insufficiency was mild.
The echocardiographic follow-up confirmed the proper function of the prosthesis and its stability (Figure 1E). Nine months after the procedure, the patient was diagnosed with a bone tumor with pulmonary metastases, a chest computed tomography revealed the position of both prostheses (Figure 1F), which had not changed since their implantation.
Malposition and migration of aortic prostheses are complications that have been reported previously;2,3,4 attempting to retrieve it or move it to the descending aorta have been proposed as the most safe alternatives. However, in the case presented here, we show that it is safe to leave a prosthesis in the ascending aorta if it is stable and does not compromise the flow in the supraaortic vessels.
Corresponding author: cruzgonzalez.ignacio@gmail.com