To the Editor,
We present the case of a 46-year-old woman with a history of dyspnea on effort. As part of the dyspnea study we first performed a coronary angiography in which it was possible to see stenosis of intermediate severity of the left anterior descending artery. An isotopic stress test showed ischemia in the territory of this artery; therefore, a coated coronary stent was then implanted on a second round cath. Due to the persistence of dyspnea, we requested a stress echocardiogram to assess functional capacity and haemodynamic behaviour during effort. The baseline electrocardiogram (ECG) (Figure 1A) showed sinus rhythm with normal intraventricular conduction. In the baseline ultrasound, the left ventricle had normal dimensions and normal global and segmental motion, and no mitral regurgitation was observed. During exercise echocardiogram, at 75 W and with a heart rate of 120 bpm, there was a left bundle branch block (LBBB) seen on the ECG (Figure 1B) and the patient had dyspnea that made it necessary to end the test. On the echocardiogram abnormal interventricular septum movement was seen due to the LHBB and severe mitral regurgitation. Three minutes after recovery the ECG and echocardiogram were normal. The subsequent analysis of myocardial deformation showed a pronounced mechanical asynchrony of the myocardial segments in which there are papillary muscle insertions, with 130 ms of delay in peak longitudinal deformation (Figure 2). A new coronary angiography ruled out in-stent restenosis, or coronary lesions. The patient was treated with betablockers and ivabradine and evolved satisfactorily, so it was decided not to implant a resynchronising pacemaker at this time.

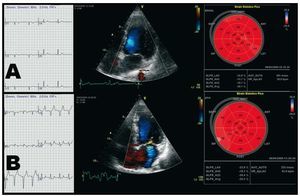
Figure 1. Electrocardiogram, Doppler colour and echocardiogram bull's eye plot with a quantitative analysis of left ventricle segmental longitudinal myocardial deformation. A: at rest: sinus rhythm with no alteration of intraventricular conduction, correct coaptation of the leaflets with no mitral regurgitation and systolic peak values of longitudinal systolic deformation within normal limits. B: stress: sinus rhythm with left bundle block, severe mitral regurgitation and peak systolic values of longitudinal systolic deformation also within normal values.

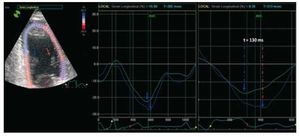
Figure 2. Analysis of left ventricle myocardial deformation in the apical plane of 2 chambers at rest (left) and during exercise (right). A synchronous deformation is seen at rest of the mid-inferior (green) and mid-anterior (blue) segments, whereas the image during exercise shows a clear delay (130 ms) at the peak of systolic deformation of both segments, which indicates that there is mechanical asynchrony.
Heart pumping function requires synchronous mechanical activation. Electromechanical asynchrony can alter the heart contraction pattern. Left bundle block is an example of ventricular asynchrony related to functional mitral failure.1,2 Functional mitral failure in patients with left bundle block has multiple components. Including, asynchrony of the papillary muscles due to delay in ventricular conduction, that causes a delay in the contraction of the papillary muscles.3,4 The delayed movement of certain areas of the left ventricle (lateral wall or interventricular septum) leads to a reduction in the force of mitral valve closure due to the fall in systolic volume caused by the asynchronous mechanical contraction.
During the last decade there has been a lot of interest in the relationship between functional mitral regurgitation and mechanical asynchrony, since by means of resynchronisation therapy it is possible to improve mitral regurgitation qualitatively and quantitatively in patients with both ischaemic and non-ischaemic cardiopathies.5 The case we present is of double interest: on one hand, proof of a relationship between ventricular asynchrony and functional mitral failure in a patient without systolic dysfunction or baseline alterations of their ventricular geometry, and, on the other, the usefulness of techniques that analyse myocardial deformation using ultrasound and make it possible to perform a detailed evaluation of the ventricular sequences of mechanical activation.