To the Editor:
Complete occlusion of the left main coronary artery (LMCA) is an extremely serious entity, with very few patients surviving this condition. In certain circumstances, the patient may survive long enough to undergo angiography.1 Following angiographic confirmation, percutaneous treatment may be undertaken. From May 2003 to December 2005, our 2 centers saw 225 patients with LMCA disease treated with drug-eluting stents, 2 (0.8%) of which initially showed complete occlusion of the LMCA on angiography. Both patients had protective collateral circulation. One of these patients, a 75-year-old man, presented with non-Q-wave myocardial infarction and the other, a 57-year-old man, with angina of recent onset. In the first (Figure 1), LMCA occlusion was considered chronic (10 days post-event). The second had subacute occlusion that became complete during catheterization. The same procedure using a guidewire and balloon was applied in both patients to unblock the LMCA, confirming bifurcation involvement. In the first, a complex technique was required, with implantation of 2 drug-eluting T stents, and in the second, good angiographic results were achieved by placement of a single stent directed toward the left anterior descending artery, with subsequent balloon dilatation of the circumflex ostium.2 Following percutaneous treatment, the clinical progress was favorable in both patients, who remained under medical supervision and were asymptomatic after 7 and 10 months of follow-up, respectively. The second patient underwent angiographic and ultrasonographic re-evaluation during follow-up. Both the angiography and ultrasound study showed excellent clinical progress of the treated segments (Figure 2).

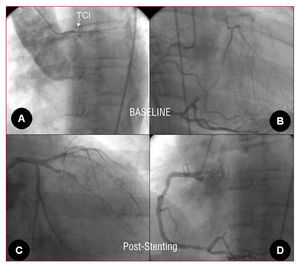
Figure 1. Baseline. A: angiography showing complete occlusion of the left main coronary artery (arrow). B: right coronary angiography, with filling of the entire left coronary system by collateral circulation. Post-stenting. C: post-stenting left coronary angiography. D: Post-stenting right coronary angiography, in which the absence of collateral circulation to the left coronary system can be seen.

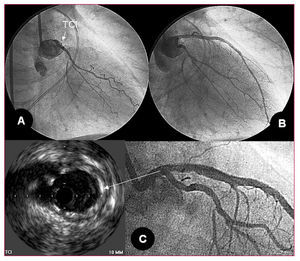
Figure 2. A: left coronary angiography after advancing a guidewire to the circumflex and balloon predilatation. B: left coronary angiography after revascularization and stent placement in the left coronary artery and anterior descending artery. C: angiography and ultrasound study at 10 months' follow-up show excellent outcome of the treated segments.
Occlusion of the LMCA is a form of arteriosclerotic coronary disease that is rarely diagnosed. The infrequency of this entity is probably due to the high incidence of associated mortality, making it unusual for patients to reach the cardiac catherization laboratory in this situation. When identified, the recommended treatment is surgery,3 when possible and the patient is seen in time. Percutaneous revascularization without dilatation in the same diagnostic procedure can be considered a second option. In general, the results obtained with bare metal stents have been promising in LMCA disease, although the high incidence of restenosis is an important limitation.4 However, following the introduction of drug-eluting stents, several studies have been published on percutaneously treated patients in whom the incidence of restenosis has considerably decreased.5-7 If this favorable long-term evolution is confirmed in ongoing studies, LMCA treatment with drug-eluting stents may become a clear alternative to surgical treatment. At present, close follow-up that includes angiographic reassessment is probably advisable. In the 2 cases of LMCA occlusion described, revascularization treatment was performed immediately after the diagnosis, with excellent initial and mid-term results.