To the Editor,
We wish to thank Escobar et al. for their letter concerning our data on ischemic heart disease in women,1 although we feel we should clarify certain points.
In our study, we did indeed observe that the women were younger, a finding that could be related to the study design per se, which involved the recruitment of patients with chronic ischemic heart disease, survivors of acute coronary syndrome who had since been stabilized; this criterion excluded the most seriously ill patients with a poorer prognosis, a population that includes the women of most advanced age.
In our article,1 we indicate that, due to the small number of women in the sample, the absence of differences in the prognosis should be assessed with caution as it may have been influenced by several factors, such as lower age or the lower prevalence of myocardial infarction and multivessel disease, as well as a shorter history of ischemic heart disease in the women (8.0±6.3 years vs 6.5±5.2 years; P<.001). Likewise, we cannot overlook the special motivation of the primary care physicians responsible for the management of these patients, which in an earlier study on heart failure (GALICAP), was shown to be a protective factor with respect to other physicians.2
With regard to the performance of fewer diagnostic tests, we agree that this could be explained by the profile of the presentation of ischemic heart disease in women.
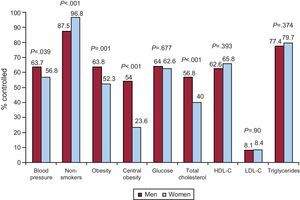
Although we had reported the degree of control of the risk factors for the overall population of the CIBAR study in a previous publication,3 we show the data, differentiated according to sex, in the Figure, which reveals a poorer control of blood pressure, obesity, and cholesterolemia in women.

Figure. Degree of control according to risk factors. HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol. Controlled blood pressure: blood pressure <140/90mmHg and <130/80mmHg in diabetes mellitus or renal failure. Obesity: body mass index <30kg/m2. Central obesity: abdominal circumference <102cm in men and <88cm in women. Glucose: <110mg/dL. Total cholesterol: <175mg/dL. HDL-C: ≥40mg/dL in men and ≥45mg/dL in women. LDL-C: <70mg/dL. Triglycerides: <150mg/dL.
Corresponding author: rafavidal@hotmail.com