Dear Editor:
Infective endarteritis was the most common cause of death in patients with patent ductus arteriosus (PDA) prior to the introduction of antibiotic therapy and surgical closure of the defect,1 though nowadays it is a rare complication.2 Infective endarteritis is especially unusual in asymptomatic patients, more so when the PDA is silent on cardiac auscultation, with very few reports of this type of case to be found in the relevant literature.3
We present the case of a 56 year old woman who had a history of PDA detected during adolescence during auscultation for a cardiac murmur. She presented to the emergency service with fluctuating fever of no apparent origin and a poor response to habitual antipyretic agents, as well as a 5 kg weight loss over 2 months.
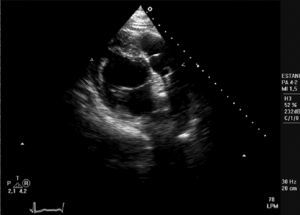
Following her admission, 3 blood cultures were positive for Streptococcus viridans. A transthoracic echocardiogram showed the left ventricle with conserved systolic function, slight aortic insufficiency, and a fixed structure on the wall of the pulmonary artery with erratic movement indicative of a vegetation (Figure). The patient was diagnosed with subacute bacterial infective endocarditis and treatment was started with penicillin G and gentamicin.

Figure. Transthoracic echocardiogram (parasternal short axis) showing the artery and pulmonary valve with a fixed structure on the arterial wall that indicates the presence of a vegetation.
The course of the patient was initially satisfactory. Ten days after admission she had another fever peak accompanied by a pleuritic type pain in her left side. A chest radiograph showed increased density in the lower lobe of the right lung. A further transthoracic echocardiogram revealed the disappearance of the vegetation that had been seen previously. A suspicion of pulmonary embolism, of probable septic origin, was confirmed by means of ventilation-perfusion pulmonary scintigraphy. A diagnosis of subacute bacterial endarteritis on PDA was confirmed, complicated by septic pulmonary embolism. Antibiotic therapy was continued with penicillin for 4 weeks and gentamicin for 2 weeks. The patient was discharged from the hospital pending closure of the PDA.
The incidence of PDA has increased spectacularly over the last 20 years, due to the increase in the survival of premature infants. The incidence is currently in the range of 0.02%-0.04% of live term births.4 The most common complications associated with PDA are left heart failure and infective endocarditis (endarteritis).1
Surgical or percutaneous closure of the PDA is indicated in practically all cases, except in those patients who have developed severe, irreversible pulmonary hypertension or in those whose PDA is silent (asymptomatic patients or with no audible murmur). Patients should also undergo surgery if they have had an episode of endarteritis.5,6 In patients with a small, asymptomatic PDA that is audible on auscultation, closure is controversial and no clear recommendation exists in the clinical practice guidelines.6-8
The case reported here concerned a patient with a small, asymptomatic PDA, with no previous risk procedure, who developed infective endarteritis, complicated by septic pulmonary embolism. Thus, infectious endarteritis is shown to be able to appear as a complication of PDA, although it is exceptional in asymptomatic patients. As the case reported shows, the risk for infection is present even in small, asymptomatic ducts, and prophylactic closure of the PDA should be considered.