To the Editor:
Persistent left superior vena cava (LSVC) is one of the most common anomalies of the thoracic venous system, being observed in 0.47%1 to 2.5%2 of the general population and up to 10% of patients with congenital heart disease.1,3 The existence of this anomaly can pose particular difficulty when introducing pacing electrodes in the heart chambers. We recently saw an 83-year-old man with revascularized ischemic dilated cardiomyopathy and NYHA grade III heart failure, who showed no clinical improvement despite optimal drug therapy. The electrocardiogram showed sinus rhythm with complete left bundle branch block, PR 185 ms, and QRS 140 ms. Echocardiography revealed a dilated left ventricle (66/51 mm), with no hypertrophy, and an ejection fraction of 33%, moderate mitral regurgitation, and an image consistent with coronary sinus (CS) dilation. A decision was made to implant a cardiac resynchronization system (CRS). After puncture of the left subclavian vein, the guidewires were seen to advance over an unusual course, descending along the left parasternal border. Selective injection of contrast material showed a persistent LSVC that drained into a highly dilated CS (Figure 1). Electrode catheters were introduced through the CS up to the marginal vein, lateral right atrium (RA), and through the RA, with a third catheter placed in the right ventricular outflow tract (RVOT) (Figure 2). The pacing and detection thresholds were verified and the electrodes were connected to a Guidant Contak Renewal generator. There were no complications during the procedure. The examination time was 37 min and the total duration of the procedure, 125 min. Following implantation, the patient experienced progressive improvement and was discharged after 7 days.

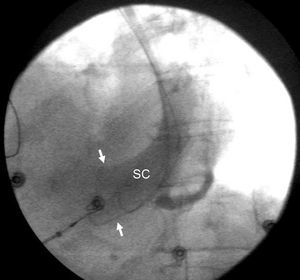
Figure 1. Venography of the left subclavian vein showing considerable dilatation (arrows) of the coronary sinus (CS).

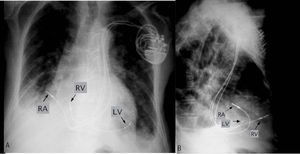
Figure 2. Chest x-ray; posteroanterior view (A) and profile view (B) that show the final position of the electrodes. LV indicates left ventricle; RA, right atrium; RV, right ventricle.
The finding of a persistent LSVC during the implantation of a pacemaker can imply additional difficulties for correct electrode placement. This is particularly important since this abnormality is occasionally associated with conduction disturbances that could require a pacemaker. Isolated cases of CRS implantation through a persistent LSVC have been published,1,3-5 with the longest series by Gasparini et al,2 including 4 cases and follow-up of 1 year. None of the patients presented complications. In the case we describe, the atrial electrode was implanted in the lateral wall because of easier accessibility, and the right ventricular electrode was placed in the RVOT using a preformed guide. Active fixation electrodes were used, as in other published cases1,3 where this system was also chosen because of instability. Although canalization of the CS is theoretically easier when there is an LSVC, selective catheterization of the veins is more difficult because they present abnormal outflows and unusual angles, and because catheter support is more unstable. In our case, the CS electrode was implanted through a conventional guide catheter directly into a marginal vein. In summary, the presence of persistent LSVC does not contraindicate safe implantation of these systems, which involves a technique with few complications.