To the Editor:
Cardiac myxomas are the most common primary neoplasms of the heart, although only 20% of cases occur in the right atrium.1
We describe a 35-year-old man, with a history of smoking and Barrett esophagus, who had presented fever of up to 38oC from 2 weeks previously, but showed no infectious foci. He also presented palpitations and tachycardia. The fever was present mainly at night and did not respond to antipyretic or antibiotic therapy. He reported similar, self-limiting fever some months earlier and asthenia from half a year previously. The systems review revealed biliuria. The physical examination also showed "straw-colored" skin, conjunctival jaundice, and jugular regurgitation. Cardiac auscultation revealed a protosystolic murmur and an audible diastolic murmur in the aortic area which were more severe at the tricuspid level. Painful hepatomegaly was found about 2 cm below the costal arch.
No significant abnormalities were observed on ECG, although the radiology showed right atrial growth. The laboratory workup revealed anemia (11 g/dL; mean corpuscular volume, 79 fL), cholestasia (total bilirubin, 2.83 mg/dL; direct bilirubin, 2.28 mg/dL; aspartate aminotransferase, 43 U/L; alanine aminotransferase, 72 U/L; γ-glutamyl transferase, 414 U/L; alkaline phosphatase, 377 IU/L), as well as elevated acute-phase reactants (α-2-globulins, 19%; erythrocyte sedimentation rate, 94 mm; C-reactive protein, 7 mg/dL; fibrinogen, 1023 mg/dL).
The abdominal sonography did not show any obstructive condition of the biliary tract, although nonspecific homogeneous hepatomegaly was observed.
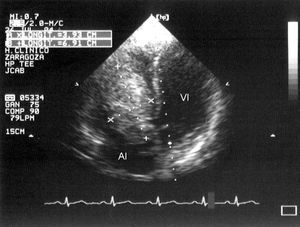
Transthoracic and transesophageal echocardiograms showed a polylobular, homogeneous mass (70x45 mm) on the tricuspid septal leaflet, with motion between the right atrium and ventricle that interfered with filling (Figure 1). The right atrium was dilated (54 mm) and showed spontaneous echo contrast in its interior; the inferior vena cava also showed physiological inspiratory collapse. The left ventricle presented abnormal motion caused by pressure overload in the right chambers and by the force of the mass on the interventricular septum. The foramen ovale was patent.

Figure 1. Mass of 69x39 mm that prolapsed into the right ventricle.
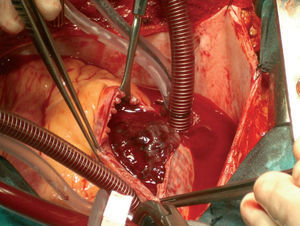
The patient underwent surgery to excise a reddish, polypous, mucoidal intra-atrial mass that had an insertion pedicle in the interatrial septum, next to the septal leaflet of the tricuspid valve, about 1 to 3 mm from the valvular annulus (Figure 2). The anatomical pathology study revealed that the lesion was myxoma.

Figure 2. Intraoperative image of the mass in the right atrium.
Progress was favorable and the patient was discharged on the sixth day after surgery. The symptoms improved in the following weeks; at 2 years the patient remained asymptomatic and with no echocardiographic signs of tumor recurrence.
Our patient presented characteristic, although nonspecific, clinical manifestations of this neoplasm (asthenia, heart murmur, and fever of unknown origin) that are described in the literature in up to 90% of cases.2 The unique aspects of our case were the clinical presentation with jaundice and elevated cholestasia enzymes due to the difficult venous return to the heart and stasis in the liver; the magnitude of the latter was related to the hemodynamic severity of heart failure.3,4 Elevated erythrocyte sedimentation rate and C-reactive protein were also present, a finding consistent with other publications.5 Normalization of these reactants after resection of the myxoma has been demonstrated.6
Echocardiography is essential for diagnosis, although transesophageal echocardiography is particularly useful in the case of atrial masses.3,5 Magnetic resonance and computed tomography will aid the differential diagnosis of intracardiac masses and provide good tissue characterization to define the extension of the tumor and its relationship to adjacent structures.3