In the article by Olry Labry Lima et al. entitled, “Cost-effectiveness and Budget Impact of Treatment With Evolocumab Versus Statins and Ezetimibe for Hypercholesterolemia in Spain” (Rev Esp Cardiol. 2018;71:1027–1035), the authors report an error in the calculation of the Markov model that affects the results reported in the Abstract, the second paragraph of the Markov Model subsection, and Table 3.
In the Abstract, where it says “To perform the 10-year Markov model, the average cost of standard treatment was 13 948.45€ vs 471 417.37€ with evolocumab.”, it should say, “To perform the 10-year Markov model, the average cost of standard treatment was €1622.63 vs €47 297.16 with evolocumab.”
In the Markov model subsection, second paragraph, where it says, “For the primary outcome, the projected mean cost of standard therapy with no discounting rate applied was €13 948.45, contrasting with €471 417.37 for evolocumab. This translates into a 10-year ICER of €1 531 434.19, which represents the projected cost of averting 1 additional cardiovascular event upon switching from standard therapy to evolocumab. Application of the 3.5% and 6% discounting rates produced ICER values of €3 101 123.88 and €4 896 643.93, respectively. For the secondary outcome, the switch from standard therapy to evolocumab incurred an additional cost of €2 171 421.91 for each averted event with no discounting. Applying the 3.5% and 6% discounting rates increased this cost to €4 090 566.86 and €6 177 284.00, respectively.”, it should say, “For the primary outcome, the projected mean cost of standard therapy with no discounting rate applied was €1622.63, contrasting with €47 297.16 for evolocumab. This translates into a 10-year ICER of €1 519 409.05, which represents the projected cost of averting 1 additional cardiovascular event upon switching from standard therapy to evolocumab. Application of the 3.5% and 6% discounting rates produced ICER values of €3 043 757.82 and €4 756 038.37, respectively. For the secondary outcome, the switch from standard therapy to evolocumab incurred an additional cost of €1 950 532.99 for each averted event with no discounting. Applying the 3.5% and 6% discounting rates increased this cost to €3 807 204.92 and €5 781 326.32, respectively.”
This correction was introduced in the electronic version of the article on December 1st, 2018.
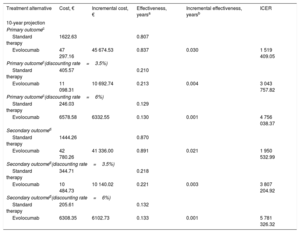
The correct Table is:
| Treatment alternative | Cost, € | Incremental cost, € | Effectiveness, yearsa | Incremental effectiveness, yearsb | ICER |
|---|---|---|---|---|---|
| 10-year projection | |||||
| Primary outcomec | |||||
| Standard therapy | 1622.63 | 0.807 | |||
| Evolocumab | 47 297.16 | 45 674.53 | 0.837 | 0.030 | 1 519 409.05 |
| Primary outcomec(discounting rate=3.5%) | |||||
| Standard therapy | 405.57 | 0.210 | |||
| Evolocumab | 11 098.31 | 10 692.74 | 0.213 | 0.004 | 3 043 757.82 |
| Primary outcomec(discounting rate=6%) | |||||
| Standard therapy | 246.03 | 0.129 | |||
| Evolocumab | 6578.58 | 6332.55 | 0.130 | 0.001 | 4 756 038.37 |
| Secondary outcomed | |||||
| Standard therapy | 1444.26 | 0.870 | |||
| Evolocumab | 42 780.26 | 41 336.00 | 0.891 | 0.021 | 1 950 532.99 |
| Secondary outcomed(discounting rate=3.5%) | |||||
| Standard therapy | 344.71 | 0.218 | |||
| Evolocumab | 10 484.73 | 10 140.02 | 0.221 | 0.003 | 3 807 204.92 |
| Secondary outcomed(discounting rate=6%) | |||||
| Standard therapy | 205.61 | 0.132 | |||
| Evolocumab | 6308.35 | 6102.73 | 0.133 | 0.001 | 5 781 326.32 |
ICER, incremental cost-effectiveness ratio, which represents the additional cost per cardiovascular event or death avoided.
This correction was introduced in the electronic version of the article on December 1st, 2018.