To the Editor:
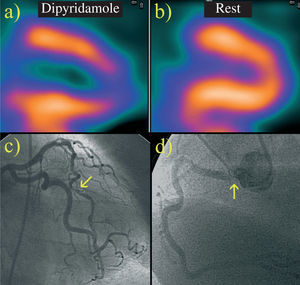
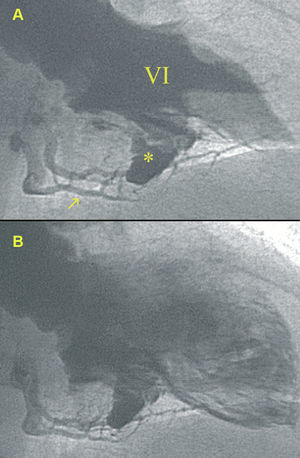
We describe a 77-year-old woman with hypertension and hypercholesterolemia who had been diagnosed with ischemic heart disease. A coronary angiography done 3 years earlier showed a lesion in the left anterior descending artery, treated with a stent, and a nonsignificant lesion in the ostium of the right coronary. The ventriculography was normal. The patient was asymptomatic for 3 years, but later consulted for recurrent angina. Single photon emission computed tomography with methoxyisobutyl isonitrile-dipyridamole showed severe anteroapical ischemia (Figure 1A and B). The coronary angiography revealed a lesion in the left anterior descending artery, a long vessel that borders the apex, no in-stent stenosis (Figure 1C), and a severe lesion in the ostium of the right coronary (Figure 1D). The ventriculography (Figure 2A and B) showed a defect (Figure 2A, asterisk) between the left ventricle and the right coronary with retrograde filling of the distal bed (Figure 2A, arrow). An interventional procedure was performed on the left anterior descending artery, and the patient progressed with no further symptoms.

Figure 1. A and B: Single photon emission computed tomography with methoxyisobutyl isonitrile-dipyridamole, vertical long axis: perfusion defect in the apical third of the anterior aspect and the apex which disappears at rest. C and D: coronary angiography: lesion in the middle third of the left anterior descending artery (C, arrow), severe lesion in the right coronary artery ostium (D, arrow).

Figure 2. Ventriculography: baseline defect (*) between the left ventricle (LV) and right coronary artery that produces retrograde filling of the distal bed (arrow) and is more evident in systole (A) than diastole (B).
In animals, myocardial circulation depends on the degree of evolution. Cold-blooded reptiles and warm-blooded mammals exhibit a spectrum of vascular patterns that generally ranges from a primitive sinusoidal pattern (where the myocardium is perfused directly from the cavity and the blood is pushed in systole to a spongy myocardium formed by a sinusoidal network in contact with the myocardial cells) to a more complex coronary type where developed arteries and capillaries perfuse a compacted myocardium.
The fetal heart of mammals initially has a sinusoidal vascular pattern.1 Afterwards, a vasculogenesis process based on differentiation of epicardial mesenchymal cells forms the right posterior and left anterior subepicardial primitive vascular network, which will produce the right and left coronary arteries, respectively.2 Angiogenesis and vascular remodeling lead to formation of the coronary arteries, which eventually connect to the aorta.1 During this process, this primitive subepicardial vascular network fails to come into contact with the intramyocardial sinusoids and, therefore, to receive blood from the ventricular chamber in normal fetal development. As the vasculogenesis process is completed, the myocardium is compacted and the primitive sinusoids disappear.
Persistent myocardial sinusoids has been described in newborns with complex congenital heart diseases.3 However, documentation of these sinusoids in the normal adult heart is extremely rare and their significance is still unknown.4 The actual prevalence and clinical relevance of this congenital anomaly, as in other coronary abnormalities, is still not well established.5
The case described shows an exceptional finding, persistent sinusoids in a normal adult heart that result in a defect between the left ventricular chamber and the right coronary. In addition, a clear, clinically important consequence of this finding can be observed: right coronary perfusion is maintained by direct vascularization from the ventricular chamber through the sinusoids, which would explain why the ostial lesion had no functional impact. The fact that this defect was not visible in the ventriculography 3 years earlier could be explained by the arteriogenesis theory6: similar to the development of mature collateral circulation from rudimentary preexisting collaterals, a persistent, latent, nonfunctional sinusoidal network becomes manifest during a process triggered by tissue hypoxia caused by epicardial stenosis. Such angiogenesis has also been observed after percutaneous laser revascularization,7 and the discovery of factors implicated in this process holds promise for future revascularization therapy in ischemic heart disease.8
As far as we are aware, this is the first report showing a clinically relevant, beneficial result of persistent myocardial sinusoids, a curious finding.
ACKNOWLEDGEMENTS
To the Nuclear Medicine Department, particularly to Dr José R. Infante de la Torre for helpful contributions to this paper.