
To the Editor:
We present the case of a patient with no structural heart disease who had complete paroxistic atrioventricular block (AVB) induced by exercise, with suprahisian block demonstrated by electrophysiology study (EPS).
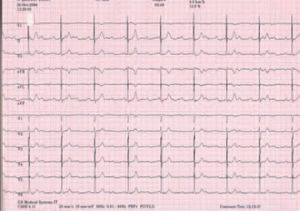
The patient, a 71 year-old, hypertense, diabetic woman with no other history of note, was referred to the emergency department with a 2-week history of asthenia and general malaise. Physical examination revealed arrhythmia, with no murmur or signs of heart failure; the remainder of the examination was unremarkable. A baseline electrocardiogram (ECG) showed Mobitz type II second degree AVB with a 3:1 conduction ratio and a narrow QRS complex (Figure 1). The only laboratory finding of note was mild hypokalemia (3.1 mEq/L). A few hours after admission the ECG was normal, with a PR interval of 216 ms and potassium concentrations of 3.6 mEq/L. Twenty-four hours after admission, however, she again suffered AVB, similar to the episode on admission, although this time the ionogram was normal. An EPS was undertaken to evaluate the distal conduction.

Figure 1. Electrocardiogram at the time of admission with Mobitz type II second degree atrioventricular block with a 3:1 conduction ratio.
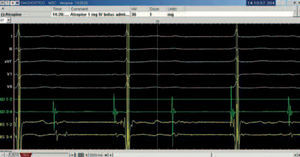
The EPS showed an HV interval of 36 ms and advanced suprahisian block, which became complete after atrial stimulation at 500 ms, as well as spontaneously, and even after the administration of 1 mg of atropine (Figure 2).

Figure 2. Demonstration of complete, suprahisian atrioventricular block. Note how each QRS complex is preceded by a hisiogram, and that the atriogram is dissociated from the hisiogram.
An ergometry test was undertaken to rule out the possibility of an ischemic origin. At the start of the test the patient was in sinus rhythm, with a normal PR interval of 68 beats per minute. After 3 minutes, and with tachycardia of 90 beats per minute, she suddenly presented a complete AVB with a heart rate of 42 beats per minute and nodal escape rhythm (Figure 3), with no chest pain. Exercise was continued until the fifth minute, when she presented widening of the QRS complex with persistence of the complete AVB, and the test was terminated. She recovered normal sinus rhythm 7 minutes after finishing the test. Coronary angiography showed absence of significant angiographic lesions. After placement of the definitive pacemaker, the patient remained asymptomatic. At the control visit 3 months after implantation of the pacemaker, complete AVB persisted with nodal escape.

Figure 3. Complete atrioventricular block during the exercise stress test.
Complete AVB induced by exercise is a relatively uncommon entity.1-5 In those cases where an EPS was carried out, an alteration of the infrahisian conduction was always detected, except in the cases with concomitant ischemic heart disease. In 1997 Rumoroso et al6 reported 4 cases and reviewed the literature. Since then, 3 new cases have been reported, with similar findings to those reported previously.7,8
The case presented here differs in some respects from the one previously reported. Firstly, the ECG on admission showed advanced, symptomatic AVB. However, unlike the other cases, most of which presented at least right bundle branch block, when our patient recovered normal sinus rhythm the ECG showed no conduction disorder or bundle branch block. Secondly, the EPS showed an alteration of the suprahisian conduction, although no test was carried out with procainamide. The disorder was seen on atrial stimulation, both spontaneously and even under the effect of atropine, which, with suprahisian involvement, should have improved conduction. This finding suggests that the adrenergic effect induced during exercise could, perhaps, itself have reproduced the block. Thirdly, the presence of a ventricular escape rhythm during the exercise stress test suggests that during adrenergic discharge not only the suprahisian conduction, but also the distal conduction was affected, when this could not be demonstrated during the EPS. Finally, the finding of a normal coronary arteriography rules out an ischemic etiology,6,9 although it does not discard the possible presence of vasospasm.
Regarding the management of these patients, Rumoroso et al6 proposed individualized treatment if there were no symptoms or conduction disorders on the baseline ECG. Given that our patient was symptomatic, the decision to implant a pacemaker was endorsed by the fact that complete AVB persisted after 3 months.
The etiology of this type of bundle branch block is probably degenerative, and independent of its degree of severity, the level of the block can be either suprahisian or infrahisian. Although the prognosis varies according to the level at which the block occurs, if there are symptoms and once any reversible etiology has been ruled out, the treatment involves the implantation of a pacemaker.