Keywords
The incidence of cardiovascular disease experienced an enormous growth from 1900 to 1950. This growth was not due to the decrease in infectious diseases, but instead was a consequence of the adoption of detrimental living habits like smoking, sedentary life-style, increased consumption of fats and carbohydrates, and stress.1 Coronary artery disease can be claimed as a disease of modern civilization. If we examine the statistics, it may seem that in recent years the mortality due to coronary disease has decreased notably, but it would be more exact to say that it has been delayed by 10 years. Coronary artery disease continues to be the primary cause of death in industrialized countries (3 of 4 deaths are of cardiovascular cause2 and it is calculated that in the year 2020 this will be the primary cause of death throughout the world). This delay has taken place thanks to the use of defibrillators and the development of reperfusion therapy, from thrombolytic medication to beta-blockers and aspirin (Figure 1). Nonetheless, patients over 75 years old are hardly represented in clinical trials and doctors often do not know how to treat them. The information available on the response to treatment and mortality in patients of advanced age is insufficient. Often, results that have been obtained with younger patients are extrapolated to the elderly and they fail to represent clinical behavior adequately.3 Finally, smoking is extending throughout the third world like an epidemic, in spite of being one of the main risk factors for cardiovascular disease. This is a socioeconomic and cultural situation that will undoubtedly have devastating consequences.

Fig. 1. Short-term mortality due to myocardial infarction in the U.S.A. in the 1962-1997 period. The period before 1962 is the era preceding the establishment of coronary units, when the mortality due to myocardial infarction was about 30%. The period from 1962 to 1984 corresponds to the development of coronary units; in this period, the use of defibrillators and hemodynamic monitoring was accompanied by a significant reduction in mortality. However, it was not until 1984, with the full development of reperfusion therapy, that an authentic decrease in the rate of mortality associated with acute coronary syndromes took place. (Taken from Braunwald et al.1)
Since it has been recognized that the incidence of coronary artery disease, far from decreasing in the population, is associated with modern living habits and is extending to more depressed regions and to progressively older patients who respond worse to treatment, we are confronted with three main challenges to detaining the advance of this epidemic: a) the need to support research; b) educate the population, and c) unify scientific language with respect to disease prevention.
FINANCING AND SCIENTIFIC STRATEGY FOR THE DEVELOPMENT OF RESEARCH
Research prolongs the life expectancy of patients and has a positive economic impact on society because it increases the productivity of the community, as can be understood from a study published recently by a group of U.S. economists. This is the main reason why many countries, including Japan, Australia, New Zealand, China, and the U.S., have decided to double the budget for research in the last 2 or 3 years. The evolution of the budget managed by the U.S. National Institutes of Health from 1993 to 2002 is shown in Figure 2. In a 5-year period, the overall financing of investigation has doubled.4 In addition, a resolution has been passed in the U.S. Senate to provide incentives for competitive research. In addition, the U.S. receives more money from non-profit institutions than any other country, and the amount of these donations has increased considerably in recent months. It should also be considered that the country´s fiscal policy of tax breaks is extraordinarily favorable to industries that invest in investigation, an economic strategy that generates enormous benefits. These points indicate that investigation addresses social and economic needs, and show that only an active policy of incentives to development and competition can create the conditions in which it is possible to benefit from the advances made.

Fig. 2. Evolution of the overall budget of the U.S. National Institutes of Health for biomedical research from 1993 to 2002. Note that in the last 5 years government authorities have decided to double the budget for this area. (Taken from Malakoff et al.4)
Another important aspect for the development of investigation is the elements that configure the scientific strategy. The person who is going to dedicate himself or herself to research must form part of a group capable of transferring the knowledge derived from basic research to applied research, which is integrated in a program of investigation that collaborates with other institutions in the public and private sectors. In addition, this group must be protected by an institution that provides the necessary infrastructure for the development of scientific activity. Nowadays, individualized research is being replaced by more integrated research, which promotes teamwork and participation in scientific programs of proven interest.
High-priority projects in cardiovascular research
The U.S. National Institutes of Health have decided that in the next 3 or 4 years one-fifth of the budget for cardiovascular research must be set aside for training new investigators, and four-fifths must be dedicated to financing research projects in the areas of vascular immunobiology, genomics and tissue transplants, and organogenesis.
In the coming years, the field of vascular immunobiology will review and change the terminology that is currently used to refer to certain pathophysiological concepts. Thus, for example, the term «atherosclerosis» will be replaced by the term «atherothrombosis», which is a much more exact denomination of this phenomenon. In 1987, Glagov et al5 described the excentric growth of atherosclerotic disease, which can produce vessel stenosis at an advanced stage. Today we know that there are two forms of presentation of atherosclerotic disease: intimal and medial. When the plaque grows excentrically, the medial layer atrophies and then develops fibrosis. On the other hand, the intimal layer can experience a parallel atherosclerotic development. At a given moment the internal elastic layer is disrupted and these two pathological processes come into contact with each other. The intimal decompression that occurs then favors plaque rupture.
In turn, the concept of «vulnerable plaque» is going to be replaced by the term «high-risk plaque». Atherosclerotic disease is a diffuse process and it is more appropriate to refer to the degree of involvement instead of plaque location, because plaques that are highly stenosing and fibrotic, such as carotid plaques, may be highly vulnerable.
Another new concept that is being introduced in the field of vascular immunobiology is that of «blood risk factors». Thirty percent of the patients who suffer myocardial infarction do not have vulnerable plaques, and plaque rupture has not been described. It seems to be related to the presence of risk factors present in the blood6 of diabetics, smokers, or patients with high cholesterol concentrations, which increase blood thrombogenicity. Tissue factor and reactive protein C are risk factors that are related to this phenomenon. It is possible that a number of plaque ruptures occur, but that only the plaque ruptures that take place in the presence of certain factors that favor blood hypercoagulability can cause myocardial infarction.
Finally, the concept of «high-risk patient» is being introduced, which can more easily be identified with imaging techniques and circulating marker levels. Magnetic resonance imaging allows us to identify the type of plaque and even to visualize 1-mm blood clots and specifically marked platelets. This means that we are entering a new era of diagnostic imaging techniques, which will contribute to the structural and molecular characterization of atherosclerotic lesions.
Research related with genetics and genomics is a high-priority field for the U.S. National Institutes of Health. It is possible that in the near future the genetic profile of an individual will identify his or her susceptibility to suffer certain diseases (Figure 3).7 Knowledge of the genes and their relation with the incidence of pathological conditions can make it possible to act with more specific and appropriate drugs, thanks to the development of the new specialty, pharmacogenetics. We know that cardiac diseases are multigenic and that the characterization of the genes involved in their development is an extraordinarily complex field of research. The type of plaques that break or the incidence of sudden death, for example, are phenomena that have particular genetic characteristics. Identification of the genetic component can facilitate prevention and treatment. Likewise, gene therapy is a field that is in continuous expansion and presents a promising future for the therapeutic approach to numerous diseases with a genetic component, although it will be many years before we benefit from the systematic use of such treatments in patients.

Fig. 3. Results of the MPHSII study of survival in coronary artery disease in male smokers or ex-smokers in accordance with the lipoprotein apo-E (isoform E4+) genotype. Smokers with this genetic profile (E4+) have a significantly worse survival than those who do not present this genotype. This is an example of how knowledge of the expression of different genotypes can help to predict the prognosis of certain conditions. (Taken from Humphries et al. Lancet 2001;358: 116-9.)
Cellular transplantation and necrotic tissue regeneration using undifferentiated cells are, perhaps, the field of investigation with the greatest potential for application soon. The transplantation of modified cells from bone marrow to regenerate the infarcted myocardium8 and the transplantation of skeletal myoblasts to replace fibrotic myocardium9 in different experimental models have already been described. Given this background, it can be foreseen that within a few years cells from the bone marrow of newborn individuals will be stored in tissue banks for use later in life. Beyond the ethical debate about the use of human embryos for obtaining tissue, studies have demonstrated that stem cells can be obtained from bone marrow and other organs of adults and used for therapeutic purposes. Recently, a study published by the Nadal group10 demonstrated that cardiac myocytes in the zone edging on an infarction have intense mitotic activity. Likewise, the understanding of different stages of vascular development is making it possible to create blood vessels in vitro.11
POPULATION STUDIES AND SYSTEMS OF PREVENTION
The implementation of preventive and educational systems targeting the community is a pending subject in our specialty. Unfortunately, we are currently treating patients but we are not preventing the disease. In Figure 4 is shown a pyramid that represents the spectrum of prevention of acute coronary syndromes. The base of the pyramid is constituted by a broad strip of the population that is at risk of suffering cardiovascular disease, and the tip of the pyramid, by subjects that have already suffered an acute coronary syndrome.12 The implementation of prevention systems in the general population is complicated, precisely due to the heterogeneity of risk factors found in different strata of the community. In recent months, numerous articles have appeared that identify new risk factors and propose drastic control measures, which often are difficult to put into practice. Thus, for example, the ATP III study postulates optimal levels for low-density lipoprotein (LDL), below 100 mg/dL, total cholesterol, below 200 mg/dL, and high density lipoprotein (HDL) levels, below 40 mg/dL.13 Nonetheless, the question we must ask is: should we treat patients who have only one risk factor, for example, an elevated concentration of homocysteine in plasma? We know that aspirin reduces the risk of coronary artery disease by 30% in the general population, but in the case of persons with a low cardiovascular risk, the probability of hemorrhage due to prolonged treatment with aspirin is much greater than the expected prevention benefit. The same occurs with the statins, which are too expensive to administer systematically to the general population. There is little information in the literature on the treatment that should be administered when a patient has a single risk factor,14 but in these cases I recommend prudence, in order to avoid overtreating patients with risk factors whose clinical impact is difficult to prove (Figure 5).

Fig. 4. Population pyramid of the spectrum of prevention with strata representing different sectors of the population and their risk of suffering acute coronary syndromes. Studies have demonstrated that certain primary prevention measures can have an important impact on the future development of coronary atherosclerosis. (Modified from Fuster.12)

Fig. 5. Classification of risk factors by their importance. The treatment of factors included as conditional risk factors should be considered only if associated with other risk factors (major or predisposing). (Taken from Fuster et al14.)
Patients need a precise numerical estimate, in the degree to which this is possible, of their true risk of developing an acute coronary syndrome, not just advice about the need to lose weight or stop smoking. Nowadays we know that if the patient has atherosclerotic disease or an equivalent risk factor (diabetes), the risk of suffering a coronary event within 10 years is more than 20%. In such patients we should aggressively reduce LDL levels (below 100 mg/dL). In contrast, persons with two or more risk factors can benefit from a less aggressive therapy to reduce LDL levels (below 130 mg/dL). It is very important to stratify risk into categories that allow an appropriate therapeutic strategy to be adopted to the needs and risks of each patient.13 The numerical quantification of risk and its clinical consequences is information that should be provided to patients for the purpose of improving the effectiveness of prevention measures.
The latest clinical studies demonstrate that in subjects with high cholesterol concentration, low HDL concentration, and high triglyceride concentration, any one of these three factors can be treated separately with beneficial results overall. Consequently, the least resistant therapeutic target can be selected for treatment. From the findings published in recent years, we can affirm that under ideal circumstances the chronic patient should be treated simultaneously with aspirin, statins and angiotensin-converting enzyme inhibitor (ACEI). However, this can only be done effectively when all three active principles are contained in a single pill. These considerations are also applicable to patients with non-coronary atherosclerosis.
Even in the low-risk population, the control of certain risk factors has been shown to have a major impact on the incidence of cardiovascular disease and cerebrovascular accidents in the community. According to the study by Hennekens et al,15 smoking cessation in the low-risk population reduces the incidence of coronary events by 50%. Similarly, a 10% reduction in plasma cholesterol levels reduces the incidence of cardiovascular disease by 30%, and a decrease of 6 mm Hg in diastolic pressure is accompanied by a 16% reduction in the incidence of cardiovascular disease and a 42% reduction in the occurrence of cerebrovascular accidents.
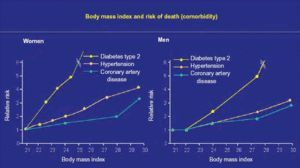
Another risk factor worth mentioning is obesity, a major epidemic of our times. Abundant evidence indicates that the impact of obesity on mortality is enormous (Figure 6). The body mass index should a parameter familiar to all of us, but it still is not attributed its true importance.

Fig. 6. Correlation between body mass index and risk of death in patients (men and women) with some of the following major risk factors: diabetes type 2, hypertension, and coronary artery disease. Note that high body mass indices are associated with an important increase in relative risk, especially among diabetic subjects. (Taken from Willet WC et al. N Engl J Med 1999;341:427-34.)
Altogether, the results of the prevention of cardiovascular disease have been fairly poor to date. If more effort were made at a governmental level to improve the eating habits of the community and control the production and use of tobacco, the socioeconomic consequences in terms of health would be very positive. But beyond what politicians can do, if each of us were to control the risk factors of some of the people around us, this probably would have an important statistical impact on the prevention of cardiovascular disease in the general community.
Correspondencia: Dr. V. Fuster, MD.
Mount Sinai Medical Center.
1 Gustave L. Levy Place - Box 1030. New York, NY 10029-6574. USA.