To the Editor:
Interest in surgical repair techniques as an alternative to valve replacement has been revived by improved knowledge of valve diseases and the possibility of more accurate assessment of their severity and origin with noninvasive techniques. Mitral valve replacement surgery is used systematically, but surgeons have less experience with the aortic valve.
This letter presents the case of successful repair of valve prolapse that was causing aortic regurgitation, with particular emphasis on the use of echocardiography for diagnosis and evaluation of the outcome of surgery.
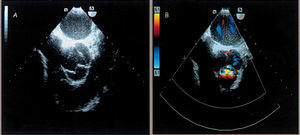
Our patient was a 62-year-old man diagnosed with severe asymptomatic aortic valve regurgitation. He did not meet the echocardiographic criteria for surgery and he had presented with grade II/IV dyspnea in the previous few months. Further echocardiographic assessments revealed an aortic valve with thin leaflets that opened normally but showed extensive right-coronary leaflet prolapse during diastole, giving rise to an off-center regurgitation jet flowing towards the anterior mitral valve. The jet was more than 12 mm wide in the long-axis parasternal view, exceeded more than 50% of the diameter of the left ventricular outflow tract, and had a vena contracta of 8 to 9 mm and a large proximal isovelocity surface area. The left-ventricular end-diastolic diameter was 45 mm (26.47 mm/m2) and the ejection fraction was 66%. The diameter (19.41 cm/m2) and structure of the ascending aorta were normal. Holodiastolic flow reversal was found in the pulsed Doppler examination. A transesophageal echocardiogram was done to assess the possibility of surgical repair. Prolapse of the right coronary cusp was observed in the transverse midesophageal view at 63º, with the leaflet appearing elongated and thin, whereas the other leaflets showed no signs of calcification and appeared normal (Figure 1A). The color-Doppler images showed a region of severe regurgitation (1.47 cm2) (Figure 1B). The remaining images added no further information to that obtained from the transthoracic echocardiogram. The anatomic structure of the aortic valve was such that surgical repair could be done by triangular resection and plication of the right coronary leaflet. According to intraoperative transesophageal echocardiography (blood pressure, 90/60 mm Hg; heart rate, 50 beats/min), no prolapse was present (Figure 2A), but a minimal central jet of grade I/IV could be discerned (Figure 2B). No complications arose after the operation. The findings of a further echocardiographic examination after 6 months were similar to those of the postoperative control. The patient was stable, and in New York Heart Association functional class I.

Figure 1. Transesophageal echocardiography, transversal view at 63º. Prolapse of the right coronary cusp (A). Severe aortic regurgitation detected with color-Doppler imaging (B).

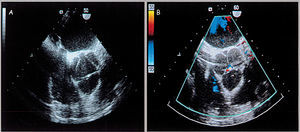
Figure 2. Intraoperative transesophageal echocardiography. Valve structure after triangular resection and plication of the right coronary leaflet (A). Color-Doppler study that only detected minimal residual aortic regurgitation (B).
In most cases, valve prolapse is associated with aortic root disease or occurs after aortic repair surgery,1,2 or with congenital diseases, such as ventricular shunts or bicuspid valve. Less often, it presents as isolated disease of 1 of the 3 leaflets, as was the case here.
Studies of aortic valve repair tend to include patients with chronic aortic dissection, annuloaortic ectasia, or congenital disease. When valve disease is isolated and not associated with the aforementioned conditions, the role of repair is not well defined. The surgical repair technique used depends on the functional classification of aortic valve regurgitation, possible classifications being type I (annular dilatation), type II (presence of redundant tissue), and type III (restrictive).3-5 The success of this type of intervention in the short-to-medium term is similar to that obtained with protheses, homografts, and autografts. Although surgical repair enjoys less success than valve replacement, it is a valid option for certain patients.3-5 According to the findings from the largest series of patients undergoing aortic valve repair, survival at 7 years after surgical repair is 89% and repeat intervention is necessary in 15% of the patients.4,5 Nevertheless, further investigation of the long-term success of the intervention is needed, and controlled studies should be done to establish whether earlier surgical indication could prevent left ventricular deterioration.6
Finally, we would like to emphasize the current role of echocardiography in the assessment of valve disease. This technique should not only be used to establish criteria for surgery but also to perform a more detailed analysis of the valve structure that would allow suitable selection of candidates for this type of procedure.