To the editor,
Adenosine (ADO) is a natural ribonucleoside that was approved for therapeutic use by the American Food and Drug Administration at the beginning of the nineties thanks to its excellent pharmacokinetic properties.1 Exogenous ADO interacts with its A1 receptor, present in sinoatrial and atrioventricular (AV) nodes, via a G1 protein. This interaction activates a specific rectifying current (lK-ADO) which hyperpolarizes the cell and induces a diminished response. Adenosine also binds to A2 receptors in the vascular endothelium, thereby reducing concentrations of cyclic adenosine monophosphate. This produces an antiadrenergic effect and may cause hypotension. The reduction in concentration of cyclic adenosine monophosphate is a brief and intense action, and makes ADO the antiarrhythmic therapy of choice for suppression of reentrant supraventricular tachycardias involving the AV node (paroxysmal supraventricular tachycardia [PSVT]). Efficacy is greater than 90%, and adverse effects are few, but not negligible.
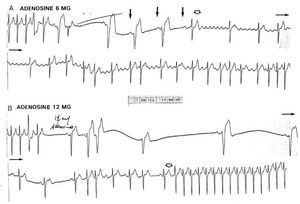
In this letter to the editor, we report an example of ADO-induced atrial instability (AI). A 72-year-old woman experienced palpitations while she was waiting for an appointment in a clinic. Figure 1 shows ECG traces recorded in the emergency department of the same hospital after administration of ADO (trace B was recorded 10 minutes after trace A). A subsequent echocardiogram was normal (left atrial diameter: 4.2 cm). AI manifest as atrial fibrillation (AF) (Figure 1A) or as atrial ectopic beats which, in turn, triggered a new episode of PSVT (Figure 1B). This second form of arrhythmia is common and self-limiting. In contrast, ADO-induced AI wich manifest as AF is uncommon (1%-12% according to studies),2,3 self-limiting, and exceptional at doses of 6 mg. Adenosine is able to induce AF by shortening the atrial refractory periods and increasing the sympathetic tone in response to action at the A2 receptors.4 The self-limited nature of the arrhythmia, which in our case occurred 3 minutes after administration, agrees with the literature. The AI that caused AF occurred during a period of relative bradycardia, in which a single atrial extrasystole (which conforms a long-short activation sequence) appeared in the vulnerable phase of atrial repolarization to trigger fibrillation. We think that this atrial substrate is similar to that in which the ventricle triggers polymorphous ventricular tachycardias (torsades de pointes) associated with prolongation of the QT interval. That is, disparity in action potential duration and voltage of atrial fibers induced by ADO, facilitated by increased sympathetic activity, favored differing responses within the atrium. We think this variation within the atrial substrate allows induction of AF at such a low dose of ADO (6 mg).

Fig. 1. Atrial instability after adenosine. A: 4.4 seconds after administration of 6 mg adenosine (central route), an atrial extrasystole, coinciding with the T wave of the prececling beat, triggers atrial fibrillation instally well organized; please note the relative sinus bradycardia (54 bm) and the long-short sequence of atrial activation (arrows). B: after 12 seconds of sinus depression and atrioventricular block atrial ectopic beats appear one of them reinitiates supraventricular tachycardia in the usual way (reentry by an accuet left accessory pathway). In A, sinus rhythm was restored 3 minutes after onset of atrial fibrillation; in B, 1 minute after. Ten minutes elapsed between A and B (see text).
The possibility of ADO-induced AF should be borne in mind. The effect will often be transient, but if the patient has a rapidly conducting AV accessory pathway, the ventricular response frequency could be dangerous. The mechanism whereby ADO induces AF (and the subsequent restauration of virus rhythm) may be of great electrophysiological and clinical interest.5